Last Updated on October 28, 2020
Split cord malformation is an uncommon congenital anomaly in which a segment of the spinal cord is divided into two parts by a fibrous or rigid bony spur.
It was previously known as diastematomyelia (diastema = a cleft, myelos = cord).
Split cord malformation can involve any part of the spinal column and sometimes involve the whole length of the canal. However, common sites of the bony spur are lower dorsal and upper lumbar regions. Rarely cases with cervical diastematomyelia have been reported. Very rarely the split cord malformation may occur without any evidence of a spur. Usually, the bony spur is attached to the dorsal surface of the vertebral body, though posterior spurs attached to hypertrophied lamina have been reported.
Split cord malformations are more common in the lower cord but can sometimes occur at multiple levels.
- 50% occur between L1 and L3
- 25% occur between T7 and T12
An associated bony, cartilaginous or fibrous spur projecting through the dura mater forwards from the neural arch is visible in 33% of cases.
Vertebral anomalies (spina bifida, butterfly or hemivertebrae) are common.
Classification of Split Cord Malformations
Split cord malformations are divided into two types according to the presence of a dividing septum and single vs dual dural sac.
Type I
Duplicated dural sac, with common midline spur (osseous or fibrous) and usually symptomatic
Type I has been further subdivided as follows:
Type Ia
Bony spur in the center with an equally duplicated cord above and below the spur
Type Ib
Bony spur at the superior pole with no space above and a large duplicated cord lower down
Type Ic
Bony spur at the lower pole with a large duplicated cord above
Type Id
Bony spur straddling the bifurcation with no space above or below the spur.
Type I is the classic diastematomyelia and is characterized by
- Duplicated dural sac
- Hydromyelia common
- Midline spur often present (osseous or osteocartilaginous)
- Vertebral abnormalities
- Hemivertebrae
- Butterfly vertebrae
- Spina bifida
- fusion of adjacent level laminae
- Cutaneous Abnormalities
- Skin pigmentation
- Hemangioma
- Hypertrichosis (hair patch)
Patients are usually symptomatically presenting with scoliosis and tethered cord syndrome
Type II
Type II has single dural sac containing both hemicords, impairment less marked.
Type II is milder than type I, and lack many of the features of latter
- Single dural sac and no spur/septum
- Cord divided, sometimes incompletely so
- Hydromyelia may be present
- Vertebral anomalies other than spina bless common
Patients are mildly symptomatic or may even be asymptomatic
Clinical Presentation of Split Cord Malformation
Symptoms can range from asymptomatic ones to pain, gait disturbance, motor or sensory deficits, and autonomic dysfunction.
About 20-25% of the patients remain asymptomatic and are diagnosed on investigating for the cause of associated cutaneous malformations. This is especially true with mild type II.
The symptomatic patient usually presents with progressive neurological deficits, usually with signs and symptoms of tethered cord.
- Low back pain
- Upper motor paresis of the lower limbs
- Urinary bladder dysfunction or incontinence
- Congenital scoliosis in children is frequently associated
Patients with diastematomyelia also frequently have other associated anomalies including:
- Meningocoele
- Neurenteric cyst
- Dermoid
- Clubfoot
- Spinal cord lipoma
- Hemangioma overlying spine
Imaging
Antenatal ultrasound
The presence of an extra echogenic focus in the midline between the fetal spinal posterior elements suggests split cord malformation.
X-rays
X-rays may show spina bifida at multiple levels, widening
- Multilevel spina bifida
- Widening of interpedicular distance
- Associated scoliosis
- Anteroposterior narrowing of vertebral bodies
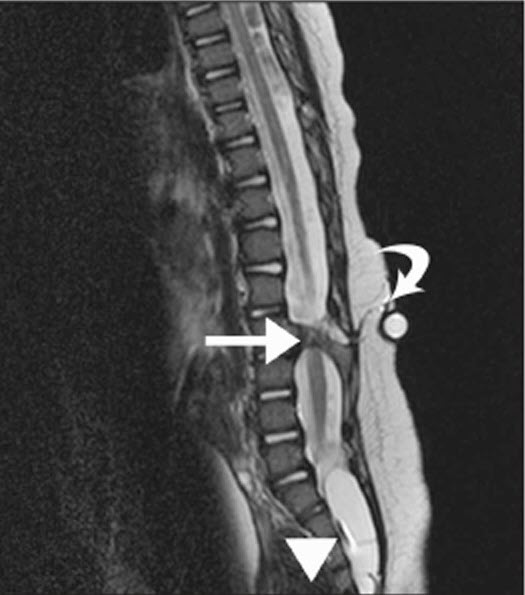
MRI
MRI is the modality of choice for assessing split cord malformations. It is able to demonstrate the cord and presence of hydromyelia along with associated anomalies.
CT
CT is able to image the bones better and is complementary to MRI.
Treatment of Split Cord Malformation
Surgery is the treatment of choice wherein the bony spur should be excised microsurgically.
The basic aim is to remove the bony or fibrous spur, division of the thick filum terminale and detethering of the cord by removal of any associated lipomas.
Low lying conus should also be addressed along with the excision of bony sp. Overall results show improvement in 40% and stable condition in more than 50% of the cases. Failure of improvement or deterioration is mostly due to incomplete removal of the bony septum.
References
- Kumar R, Singh V, Singh SN. Split cord malformation in children undergoing neurological intervention in India: A descriptive study. J Pediatr Neurol. 2004;2:21–7.
- Mahapatra AK, Gupta DK. Split cord malformations: A clinical study of 254 patients and a proposal for a new clinicoimaging classification. J Neurosurg Pediatr. 2005;103:531–6.
- Pang D. Split cord malformation II. Clinical syndrome. Neurosurgery. 1992;31:481–500. Sinha S, Agarwal D, Mahapatra AK. Split cord malformations: An experience of 203 cases. Childs Nerv Syst. 2006;22:3–7.
- Kumar R, Bansal KK, Chhabra DK. Split cord malformation in pediatric patients. Neurology India. 2001;49:128–33.
- Venkatramana NK. Split cord malformations. J Pediatr Neurosci. 2006;1:5–9.