Last Updated on October 30, 2023
Cervical spine movements are complex and result of individual vertebral motion. There are six movements possible in the normal range of motion of the cervical spine. These are
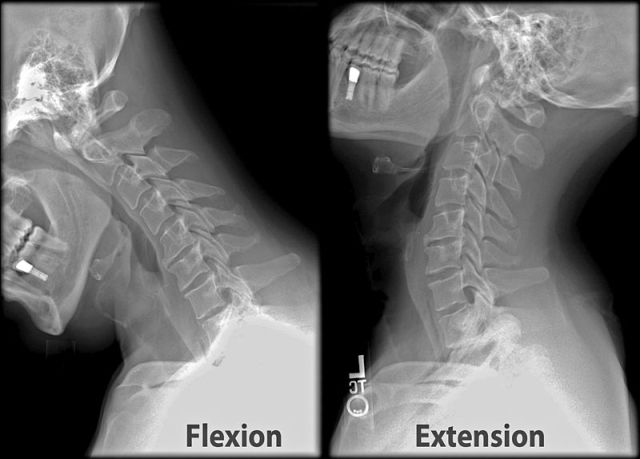
Flexion
A movement by which chin attempts to touch the chest.
Extension
A movement in the opposite direction of flexion
Lateral Flexion
This movement allows you to tilt your neck as if touch ear to your shoulder. The movement is equal on both sides.
Rotation
Rotation is the movement which we use to look over our shoulder or look back. The movement is equal on either side.
The normal cervical range of motion is
- Flexion – 80 to 90 degrees
- Extension – 70 degrees
- Lateral flexion – 20 to 45 degrees on both sides
- Rotation – 90° of rotation to both sides.
In normal daily use, the movements are hardly uniplanar as outlined above.
Normal Kinematics of the Upper Cervical Spine
Both flexion and extension movements are reported to be initiated is also initiated in the lower cervical spine.
The first cervical vertebra, the atlas, articulates with the occipital condyles, and its primary motions are flexion and extension.
Normal flexion to hyperextension at the atlanto-occipital joint range is 15 to 20 degrees. Rest is contributed by lower vertebrae.
Rotation and lateral flexion between the occiput and atlas are not possible due to the depth of the atlantal sockets. These movements occur on atlantoaxial joint [C1-C2].
The C1-C2 motion segment accounts for 50% of the rotation in the cervical spine.
The normal ranges of rotation of C1 on C2 are reported to be 50° to each side. Rotation of the atlas on the axis does not occur without a small degree of extension and lateral flexion and sometimes flexion.
Cervical spine flexion and extension often create motion in the direction opposite that being experienced in the atlas. Thus, when the cervical spine is flexing, the atlas extends, and when the cervical spine extends, the atlas flexes.
The orientation of the cervical vertebral bodies of the mid to lower cervical column allows for rotation and flexion movements but is resistant to lateral flexion. Lateral flexion is possible in the cervical column but only due to coupled rotational movement in each segment to that side.