Last Updated on October 27, 2023
The ankle joint is a hinged synovial joint. In an absolute sense, its primary movements are moving the foot up and down, called dorsiflexion and plantar flexion respectively.
However, this joint works in tandem with subtalar joints [talocalcaneal and talocalcaneonavicular], thus adding to the range of motion of this ankle-subtalar joint complex.
Anatomically subtalar (talocalcaneal) joint refers to the articulation between the talus and the calcaneus. However, in the functional sense subtalar joint means the talocalcaneonavicular joint as two joints – talocalcaneal and calcaneonavicular, do not function independently.
Structure of Ankle Joint
The ankle joint is the synovial joint of the hinge variety.
The superior articular surface of the joint, a kind of deep socket is formed by articular surfaces of
- The lower end of the tibia including the medial malleolus
- Lateral malleolus
- Inferior transverse tibiofibular ligament
The inferior articular surface is formed by articular areas on the upper, medial and lateral aspects of the talus.
Stability of Ankle Joint
The ankle joint is a strong joint made stable by
- The close interlocking of the articular surfaces
- Strong collateral ligaments on the sides
- The tendons that cross the joint (four in front, and five behind)
- The depth of the superior articular socket is contributed to by
- The downward projection of the medial and lateral malleoli
- The transverse tibiofibular ligament
- Bridges across the gap between the tibia and the fibula behind the talus.
The socket is provided flexibility by the tibiofibular ligaments, the flexibility of the fibula, and by slight movements of the fibula at the superior tibiofibular joint.
Anatomically, two factors tend to displace the tibia and fibula forwards over the talus
- The forward pull of tendons passes from the leg to the foot;
- Pull of gravity
But following factors are responsible for prevention of displacement
- The talus is wedge-shaped, being wider anteriorly.
- The posterior border of the lower end of the tibia is prolonged downwards.
- Ligamentous structures
Ligaments of Ankle
Ligaments play an important part in ankle stability. The anterior and posterior ankle capsular ligaments are relatively thin compared with the medial and lateral ankle ligaments. Here, the stability beyond movement range is produced by bone-on-bone abutment.
The joint is supported by a fibrous capsule, the deltoid or medial ligament, and a lateral ligament.
Fibrous Capsule
It surrounds the joint and is attached all around the articular margins with two exceptions
- Posterosuperiorly, it is attached to the inferior transverse tibiofibular ligament
- Anteroinferiorly, it is attached to the dorsum of the neck of the talus at some distance from the trochlear surface.
The anterior and posterior parts of the capsule are loose and thin to allow hinge movements. On each side, however, it is supported by strong collateral ligaments.
The synovial membrane lines the capsule. The joint cavity ascends for some distance between the tibia and the fibula.
Medial Ligaments
Deltoid Ligament
This is a very strong triangular ligament present on the medial side of the ankle. The ligament is divided into a superficial and a deep part.
The superficial deltoid ligament originates from an anterior bony prominence of the medial malleolus referred to clinically as the anterior colliculus. It spreads to form three portions
- Most anterior part is the tibionavicular which inserts on to the navicular
- The middle, tibiocalcaneal part inserts onto the sustentaculum tali
- The posterior fibers form posterior tibiotalar ligament and are attached to the medial tubercle and to the adjoining part of the medial surface of the talus.
The deep deltoid ligament originates from the intercollicular groove and a posterior bony prominence referred to clinically as the posterior colliculus. [Both deep and superficial have an almost same place of origin].
It is shorter and thicker than the superficial deltoid ligament and is contiguous with the medial capsule of the ankle joint and the medial portion of the interosseous talocalcaneal ligament. It is attached to the anterior part of the medial surface of the talus.
The deltoid ligament is crossed by the tendons of the tibialis posterior and flexor digitorum longus.
The greatest mechanical forces across the ankle joint are directed medially in the normal external rotation of the foot in walking and running. That is why the medial ligaments are thicker.
The deltoid ligament primarily prevents abduction and acts as a secondary restraint against anterior translation. The deep deltoid ligament provides the greatest restraint against lateral translation.
Complete rupture of superficial and deep deltoid ligament results in a valgus tilt of talus.
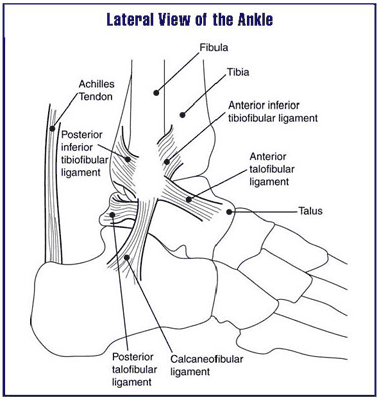
Lateral Ligament Complex
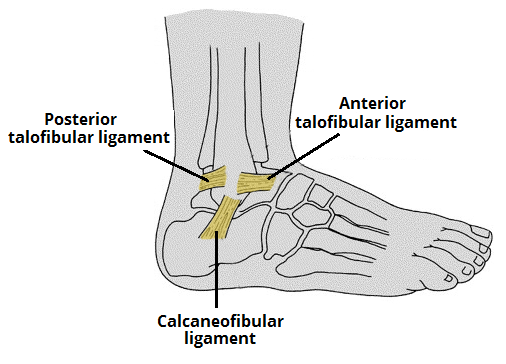
This ligament consists of three bands as follows.
- The anterior talofibular ligament
- The posterior talofibular ligament
- The calcaneofibular ligament
The anterior talofibular ligament
The anterior talofibular ligament is a flat band which passes from the anterior margin of the lateral malleolus to the neck of the talus, just in front of the fibular facet.
Anterior talofibular ligament primarily restricts internal rotation of the talus in the mortise. In plantar flexion, it also inhibits adduction.
The posterior talofibular ligament
The posterior talofibular ligament passes from the lower part of the malleolar fossa (of the fibula) to the lateral tubercle of the talus.
The posterior talofibular ligament is the strongest of the three lateral ligaments. It runs almost horizontally from the fossa in the inner aspect of the tip of the lateral malleolus to the posterior tubercle of the talus.
It inhibits external rotation with the ankle in dorsiflexion. It also assists medial ligaments in restriction of dorsiflexion.
The short fibers can also restrict internal rotation after rupture of the anterior talofibular ligament.
If the calcaneofibular ligament is disrupted, posterior talofibular ligament inhibits adduction with the ankle in dorsiflexion.
The calcaneofibular ligament
The calcaneofibular ligament is a long rounded cord which passes from the notch on the lower border of the lateral malleolus to the tubercle on the lateral surface of the calcaneum. It is crossed by the tendons of the peroneus longus and brevis.
The CFL prevents adduction.
Following ligaments are part of subtalar lateral ligament complex.
- Calcaneofibular ligament [ Thus calcaneofibular ligament spans the tibiotalar and talocalcaneal joints]
- Lateral talocalcaneal ligament
- Cervical ligament
- Interosseous talocalcaneal ligament [Provides an axis of rotation for movement of the talocalcaneal joint]
Syndesmosis of Ankle
The syndesmosis of the ankle refers to the structures connecting the tibia to the fibula. It is important because injuries to syndesmosis, called syndesmotic injury results in splaying of lower tibia and fibula.
These are
- Anterior [or anteroinferior] tibiofibular ligament
- Posterior [or posteroinferior tibiofibular] ligament
- Interosseous tibiofibular ligament –
Anterior tibiofibular ligament is most commonly injured in syndesmotic injuries
Relations of the Ankle Joint
Anteriorly, from medial to the lateral side
- Tibialis anterior
- Extensor hallucis longus
- Anterior tibial vessels
- Deep peroneal nerve
- Extensor digitorum longus,
- Peroneus tertius.
Posteriorly, from medial to lateral side
- Tibialis posterior
- Flexor digitorum longus
- Posterior tibial vessels
- Tibial nerve
- Flexor hallucis longus
- Peroneus brevis
- Peroneus longus.
Movements of Ankle Joint
Active movements are dorsiflexion and plantar flexion.
- In dorsiflexion, the forefoot is raised, and the angle between the front of the leg and the dorsum of the foot is diminished. Principal muscle involves tibialis posterior. Accessory muscles are extensor digitorum longus, extensor digitorum hallucis, and peroneus tertius.
- In plantar flexion, the forefoot is depressed, and the angle between the leg and the foot is increased. Gastrocnemius and soleus via tendoachilles are principal muscles whereas plantaris, tibialis posterior, flexor hallucis longus, and flexor digitorum longus are accessory muscles.
In dorsiflexion, the anterior talofibular ligament is loose, and the calcaneofibular ligament is taut. This is reversed in plantarflexion.
Though [lantarflexion and dorsiflexion are primary movements, biomechanically, a certain amount of motion is allowed in all planes. When the ankle goes from full plantarflexion to full dorsiflexion, the distance between the lateral and medial malleoli increases by approximately 1.5 mm. Rotation, as much as 6 degrees of the tibia on the talus can also occur while a person is walking.
Blood Supply of Ankle Joint
Ankle joint receives blood supply from branches of anterior tibial, posterior tibial, and peroneal arteries.
Nerve Supply
The ankle joint is supplied by the deep peroneal and tibial nerves.
Clinical Significance
The ankle is frequently injured, especially in motor vehicular trauma and sports injuries. The most common injury is a sprain but different pattern of fracture injuries can occur depending upon the forces acting on the joint at the time of injury.
Dislocation of the ankle is rare because the joint is very stable due to the presence of the deep tibiofibular socket. But it can accompany fracture of one of the malleoli.