Last Updated on December 25, 2023
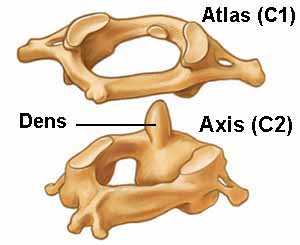
Atlas is the first cervical vertebra that sits just below the skull. It is also called C1 vertebra. Along with axis, the second vertebra and C7, it falls into the group of atypical cervical vertebrae.
Atypical because these have unique features.
Axis and C7 or vertebra prominens are discussed separately.
Atlas is unique in its shape. It articulates with the dens of the axis, a process of axis vertebra that projects superiorly and the occiput.
Articulation with axis allows rotation of the head whereas articulation with occiput assists in flexion, extension and lateral flexion of the head.
It is called the atlas after the mythological hero that bore the weight of celestial heavens on its shoulders.
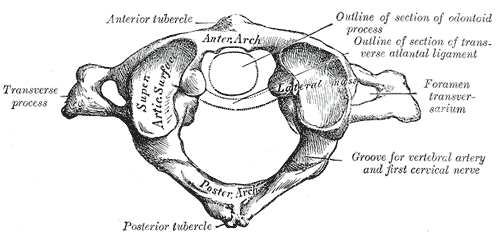
Atlas can be identified by its ring shape. There is no vertebral body or spinous process.
Structure of Atlas
The atlas is composed of
- Anterior arch marked by a median anterior tubercle on its anterior aspect. Its posterior surface bears an oval facet to articulate with the dens.
- Posterior arch – Forms three-fifths of the ring. Posterior surface is marked by the median posterior tubercle.
- Paired lateral masses
- Paired transverse processes
It has no body. The dens of the axis sits where a body of a typical vertebra is.
The transverse atlantal ligament [it holds dens against the anterior arch] divides its vertebral canal into anterior 1/3 and posterior 2/3. The anterior portion is occupied by dens.
The spinal cord is present in the posterior portion.
Anterior arch
It has the following important parts.
Anterior tubercle is present on the anterior aspect of the anterior arch. It is the site of attachment of the anterior longitudinal ligament
Posterior facet for the dens is prsent on the posterior aspect of the anterior arch
Upper border and lower borders provides attachment to
- Anterior atlanto-occipital membrane
- Lateral parts of the anterior longitudinal ligament
Posterior arch
It forms 3/5th of the circumference of the ring.
Posteriorly, it bears posterior tubercle which is a rudimentary spinous process. it provides an attachment to the ligamentum nuchae.
Posterior to lateral mass, the superior surface of the posterior arch has grooves for C1 nerve and vertebral artery.
Superior border provides attachment to the posterior atlanto-occipital membrane and inferior border provides atachment to ligamentum flava or yellow ligament.
Lateral Mass
These are paired ovoid structures whose upper surface bears elongated concave articular facet directed upwards and medially. This articular facet articulates with the corresponding condyle to form an atlanto-occipital joint.
On the lower surface, there is an articular facet which is almost circular, flat and is directed downwards, medially and backwards.
It forms the atlantoaxial joint with axis vertebra.
The medial surface bears a small roughened tubercle for attaching transeverse ligament ad is also marked by a vascular foramen.
Transverse Process
It projects laterally from the lateral mass and is very long. In fact, it is longer than all of the transverse processes of the cervical vertebrae except C7. [ You can palpate by insinuating finger between the angle of mandible and mastoid process.]
It, by virtue of its length, acts as an effective lever for head rotation.
The transverse process is pierced by the foramen transversarium which harbors vertebral arteries.
Sometimes. a tubercle is present on the anterior aspect of the transverse process
Joints of Atlas
Atlanto-occipital joint
This is a synovial joint between the occipital condyle and superior facet of the lateral mass of the atlas.
The joint is covered by a capsule and allows for flexion, extension and lateral flexion.
It is innervated by C1 fibers.
Atlanto-axial Joint
Atlanto-axial joint is actually composed of two types of joints. One is medial atlantoaxial joint between dens and posterior aspect of anterior arch of the atlas. Another type is lateral atlantoaxial joint, present on either side, between inferior articular facet of the atlas and superior articular facet of the axis.
Median atlanto-axial joint
- Synovial joint between the dens of the axis and the posterior aspect of the anterior arch of the atlas
- Allowsthe rotation of the head.
- The dens is held in place by the transverse ligament. there is a bursa between the two.
Lateral atlanto-axial joint
- Synovial joint between the inferior articular facet of the atlas and the superior articular facet of the axis
- Allows the rotation of the head
- Innervated by the C2 nerve
Attachments
- The anterior tubercle
- Anterior longitudinal ligament in the median plane
- Upper oblique part of the longus colli muscle
- Anterior arch
- Upper border – Anterior atlanto-occipital membrane.
- Lower border
- Lateral fibers of the anterior longitudinal ligament.
- Atlantoaxial ligament [ Provides tertiary support against ventral translation of the dens.]
- The posterior tubercle
- Ligamentum nuchae in the median plane
- Origin to the rectus capitis posterior minor on each side
- Posterior arch
- Groove on the superior surface occupied by the vertebral artery and C1 nerve.
- Behind the groove attachment to the posterior atlanto-occipital membrane.
- Lower border – Attachment to ligamenta flava.
- Lateral mass
- Tubercle on medial side gives attachment to the transverse ligament of the atlas.
- The anterior surface – origin to the rectus capitis anterior
- Transverse process
- Origin to the rectus capitis lateralis (upper surface anteriorly)
- Superior oblique (upper surface posteriorly)
- Inferior oblique (lower surface of the tip)
- Levator scapulae (lateral margin and lower border)
- Splenius cervicis
- Scalenus medius.
Thus following muscles are attached on the atlas
- Longus colli
- Splenius cervicis
- Superior oblique
- Inferior oblique
- Rectus capitis posterior minor
Anatomical Variations
- Arcuate foramen is a normal variant of the atlas and develops by calcification of the posterior atlanto-occipital membrane. It is also known as foramen arcuale atlantis, ponticulus posticus or posterior ponticle, or Kimerle anomaly. Vertebral arteries pass through this foramen. It is seen in about 8% and is more common in females. It can be unilateral or bilateral, or complete or incomplete.
- Two superior articular facets of the lateral masses anterior and posterior [instead of single]
- Absent central part of the posterior arch
- Partial or complete fusion with occiput or axis
Ossification of Atlas
- Three centers – anterior ossification center, and paired lateral mass ossification centers. [week 7]
- The paired lateral mass ossification centers extend to the posterior arch.
- Unification at the posterior arch – 3-4 years
- Anterior ossification center unites with the lateral mass ossification center at years 6-8.
- Sometimes two anterior ossification centers present.