Last Updated on November 11, 2019
Elbow pain can be due to the problem in elbow joint, bones forming the joint or the tissues surrounding it. Elbow joint is formed by humerus bone above, and radius and ulna bones below. Most elbow pain results from overuse injuries.
Relevant Anatomy of the Elbow
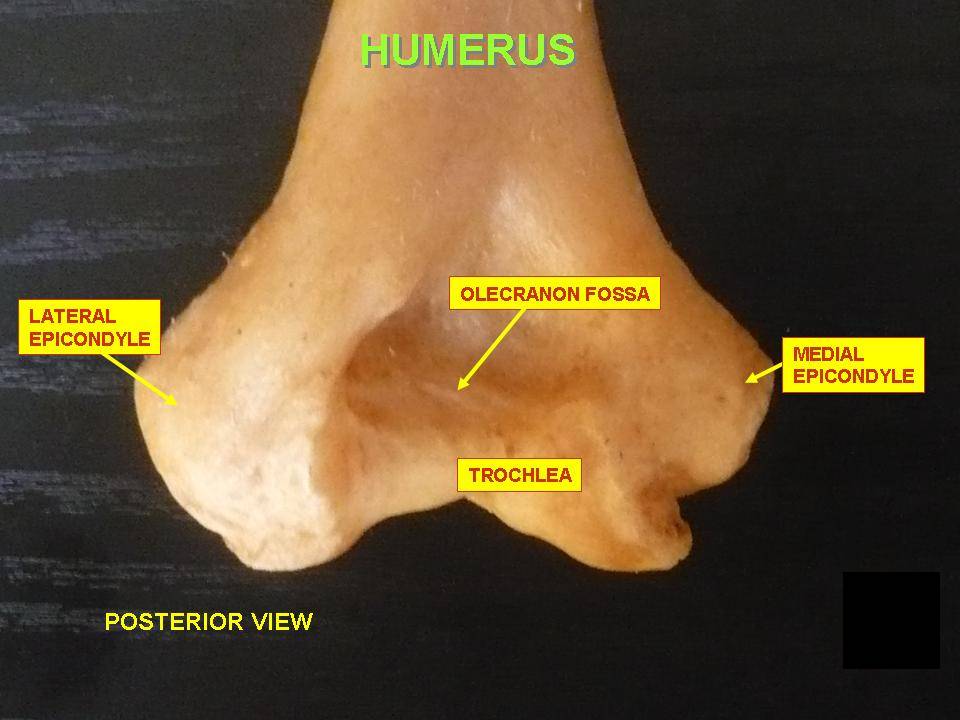
Lower End of Humerus
The lower end of the humerus forms the condyle which is expanded from side to side and has articular and nonarticular parts.
Articular parts
- Capitellum is a rounded projection which articulates with the head of the radius.
- Trochlea is a pulley-shaped surface that articulates with the trochlear notch of the ulna. The medial edge of the trochlea projects down 6 mm more than the lateral edge: this results in the formation of the carrying angle.
The Nonarticular part
- Medial epicondyle is a prominent bony projection on the medial side of the lower end. It is subcutaneous and is easily felt on the medial side of the elbow. Ulnar nerve lies posterior to this and can be palpated easily.
- Lateral epicondyle is on the lateralmost aspect of the expanded lower humerus.
- Lower lateral and medial margins are called ridges.
- Three fossae
- Coronoid fossa – Above the anterior aspect of the trochlea to accommodate the coronoid process of the ulna on flexion.
- The radial fossa is a depression present just above the anterior aspect of the capitulum and accommodates the head of the radius on flexion of the elbow.
- Olecranon fossa lies just above the posterior aspect of the trochlea and accommodates olecranon process of the ulna on the extension of the elbow.
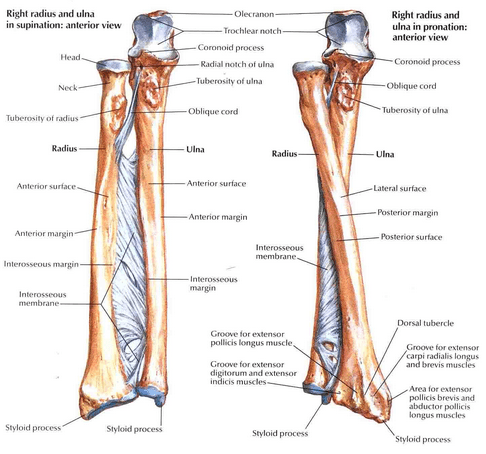
Upper End of Ulna
The olecranon process projects upwards from the shaft and its anterior surface is articular. It forms the upper part of the trochlear notch.
The posterior surface is subcutaneous and is separated from the skin by a bursa.
Inferiorly, it is continuous with the posterior border of the shaft of the ulna. The upper part forms the point of the elbow
Coronoid process projects forwards from the shaft just below the olecranon its superior surface forms the lower part of the trochlear notch. The anterior surface is triangular and rough.
The upper part of its lateral surface is marked by the radial notch for the head of the radius. The annular ligament is attached to the anterior and posterior margins of the notch. The lower part of the lateral surface forms a depressed area to accommodate the radial tuberosity. It is limited behind by a ridge called the supinator crest.
The trochlear notch forms an articular surface that articulates with the trochlea of the humerus to form the elbow joint.
The radial notch articulates with the head of the radius to form the superior radioulnar joint.
Radius Upper End
The head is disc-shaped and is totally covered with articular cartilage. It has got a concave superior surface that articulates with the capitellum of the humerus at the elbow joint. The rim of the head articulates with the radial notch of the ulna and the annular ligament, forming the superior radioulnar joint
The neck is enclosed by the narrow lower margin of the annular ligament. The head and neck are free from capsular attachment and can rotate freely within the socket.
There are two movements in elbow joint
- Flexion and extension
- Rotation
Various ligaments and muscles stabilize the elbow joint.
The biceps muscle is the major muscle that flexes the elbow hinge. The triceps muscle is the major muscle that extends the elbow hinge.
A bursa is present between the posterior surface of olecranon and skin of the elbow.
Causes of Elbow Pain
The elbow can be affected by inflammation of the tendons or the bursae, or conditions that affect the bones and joints, such as fractures, arthritis, or nerve irritation.
Lateral Epicondylitis or Tennis Elbow
 The lateral epicondyle is the lateral most part of the lower humerus and is nonarticular. It gives rise to extensor muscles of the forearm by common extensor origin.
The lateral epicondyle is the lateral most part of the lower humerus and is nonarticular. It gives rise to extensor muscles of the forearm by common extensor origin.
Tendinitis of this origin is called lateral epicondylitis, also known by the name of tennis elbow as it was noted more in tennis and other racquet sports players.
The repetitive motion of the forearm is considered to be the main cause. For example, using a manual screwdriver, washing windows, or hitting a backhand in tennis play.
The patient usually complains of pain outside of the elbow and may be accompanied by mild swelling. There would be tenderness at the lateral epicondyle region. The elbow maintains its full range of motion
X-rays are usually normal but can show calcium deposits in the tendon or other abnormalities of the elbow joint.
The treatment of tennis elbow includes
- Rest
- ice packs
- NSAIDs and other analgesics
- Local steroid injections
- supportive straps
- Surgery in severe cases
Medial Epicondylitis or Golfer’s Elbow
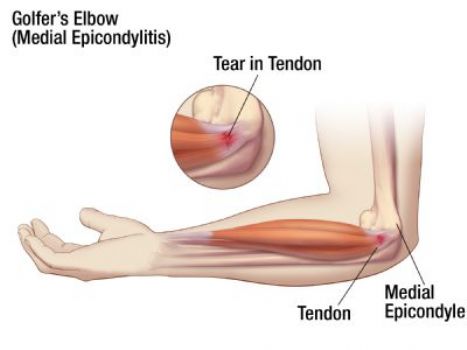
The counterpart of lateral epicondyle is medial epicondyle. Here the flexor tendons of forearm and hand originate. Inflammation of this origin is termed as medial epicondylitis and is another kind of tendinitis.
Medial epicondylitis is characterized by local pain and tenderness over the inner elbow. Activities that require twisting or straining the forearm can elicit pain and worsen the condition Rest of elbow motion is not affected.
Elbow x-rays, just like tennis elbow are normal. In long-standing cases, calcification may be present.
The treatment is on a similar line of the treatment of tennis elbow.
Read more about golfer‘s elbow
Olecranon Bursitis
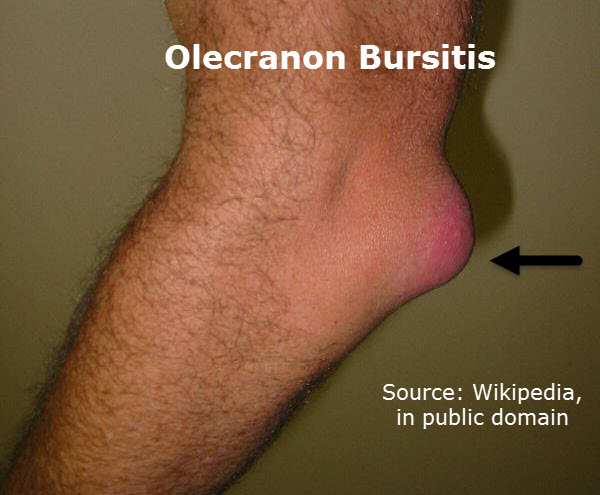
Olecranon bursitis is the swelling and inflammation of olecranon bursa. It could occur due to repetitive injury, trauma, infection or some crystal deposition diseases.
Olecranon bursitis presents with the swelling over the tip of the elbow on extensor aspect. In case of infection, there may be redness and warmth as well.
The treatment includes rest, avoidance of trauma, ice packs and anti-inflammatory drugs. In case of infection, antibiotics may be added.
[Read more about Olecranon Bursitis]
Fractures and Dislocations
Bones around elbow may get fractured, including intraarticular area. Many elbow injuries can be the cause of pain and degree of injury would vary with the degree of trauma. The patient would present with a history of acute trauma and an x-ray would show a fracture in most of the cases.
The treatment of these injuries vary depending on the fracture pattern and the type of bone involved. Generally, the treatment consists of plaster immobilization of surgical fixation. The treatment needs to be individualized and vary from case to case.
Elbow Sprain
A sprain is an injury to the ligament that results in stretch or tear. Again, this occurs following the trauma and severity of sprain would depend on the extent of the injury. The number of ligaments involved also add to severity. Treatment involves rest, ice, immobilization, compression, and anti-inflammation drugs.
Arthritis of the Elbow
There are many types of arthritis that can affect elbow. These include rheumatoid arthritis, gouty arthritis, psoriatic arthritis, ankylosing spondylitis, and reactive arthritis.
Pain is the initial complaint. There may be swelling in advanced arthritis. Joint may be tender and range of motion of joint is decreased.
The treatment includes rest initially followed by mobilization exercises, drugs for relief of pain. Medication to treat the underlying disease. In case of advanced joint destruction, surgery such as joint arthroplasty may be needed to restore joint function. In other cases, arthrodesis may be required to immobilize the joint.
Cellulitis
Cellulitis is inflammation of the skin. This may occur the following abrasion. The patient presents with pain in the affected site, warmth, redness, and swelling in the area.
The region becomes more sensitive to touch and clothes or temperature.
This may be accompanied by fever and systemic symptoms of malaise etc.
There would be an increase in leucocyte count especially neutrophils. Rest of the investigation profile should be done depending upon the individual patient.
Analgesics and antibiotics [oral or parenteral] are the standard treatments.
Infected Elbow Joint or Bacterial Arthritis
Bacterial arthritis or septic arthritis of the elbow joint is not very common and its presence should alarm to investigate for the presence of immunosuppression like diabetes, HIV, use of steroids and other drugs which may cause loss of immunity.
Intravenous drug abuse is also a high-risk factor.
The disease presents with fever, severe pain in the elbow and limitation of joint movement.
The joint is very warm, swollen. Septic arthritis of the elbow requires antibiotic treatment and surgical evacuation.
Tumors
Tumors are uncommon in elbow joint but tumors may affect the bones. Depending on the type, these could be painless or painful.
Bone scan, x-rays, and MRI and if required biopsy, are the investigations required to reach at diagnosis.
The treatment of the tumor depends on the type and site.
Similarly, other structures of the elbow like nerves, mesenchymal connective tissue and vessels may have malignancy and cause of pain in the elbow.
Ulnar Nerve Entrapment
The ulnar nerve is present on the posterior aspect of the medial epicondyle. The nerve can get pinched by normal structures or following injury.
The pain of the elbow may or may not be present. Numbness and tingling of the little and ring finger of the hand may be felt. Pain may occur in the entire forearm, usually the medial side [the side of the little finger].
Medical treatment consists of rest, anti-inflammatory and steroids.
In severe cases, surgical decompression and repositioning of the ulnar nerve can be required.