Last Updated on October 28, 2023
Humeral avulsion of the glenohumeral ligament or HAGL refers to avulsion of the inferior glenohumeral ligament (IGHL) from its humeral insertion.
When it is associated with a bony avulsion fracture, it is called as bony humeral avulsion of the glenohumeral ligament (BHAGL lesion).
Humeral avulsion of the glenohumeral ligament is often seen in young men engaged in contact sports like rugby, football etc..
It can lead to traumatic anterior shoulder instability. Though Bankart lesion (detachment of the anteroinferior labrum) is a major cause of traumatic instability of the shoulder, humeral avulsion of the glenohumeral ligament is also an important reason in roughly 7-9% of cases of primary shoulder instability.
HAGL most often results from anterior shoulder dislocation due to forced hyperabduction and external rotation of the arm.
This lesion should be considered in the presence of a known following lesions along with the absence of any other demonstrable cause of chronic shoulder instability and pain.
- Bankart lesion
- Hill-Sachs defect
- Rotator cuff pathology
Proper diagnosis and management of these lesions are critical to restore shoulder stability and function. Surgical repair is generally recommended.
Anatomy and Biomechanics
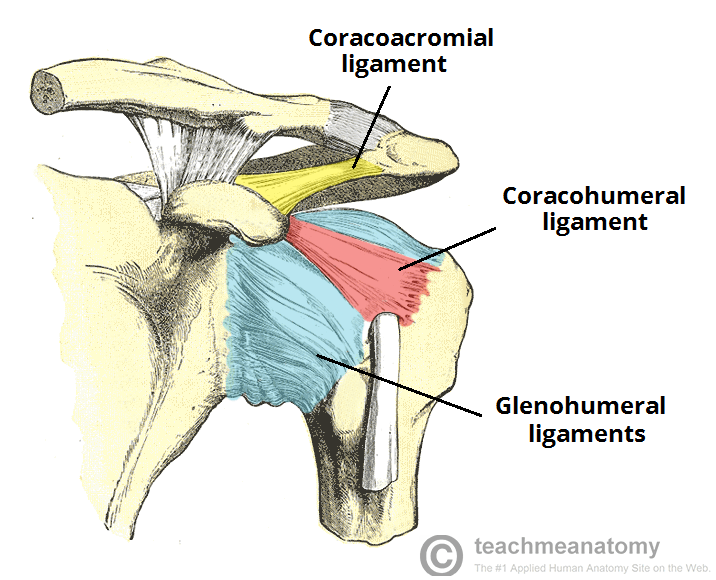
Inferior glenohumeral ligament is sometimes referred to as the inferior glenohumeral ligament complex. It runs from runs from the inferior two-thirds of the glenoid labrum and/or neck to the lateral humerus to attach on the anatomical neck of the humerus and is composed anterior band, posterior band and axillary pouch which is laxity between anterior and posterior bands
Inferior glenohumeral ligament is the most important of the three glenohumeral ligaments as it prevents dislocation at the extreme range of motion. It is the most important static stabilizer of the shoulder.
It can stretch or tear esp the anterior band, at the glenoid insertion with or without concomitant injury to the labrum and capsule. The disruption occurs at the humeral insertion or midsubstance are less common.
Inferior glenohumeral ligament is most stressed in abduction and external rotation.
There is an increased likelihood of a HAGL lesion with hyperabduction and external rotation,
The extent of the injury is often fully appreciated and diagnosed only at the time of shoulder arthroscopy.
In multiple injuries, the HAGL may go unrecognized and cause continued instability.
Clinical presentation of HAGL
Usually, there would be a history of shoulder dislocation. There would be a complaint of shoulder instability and anterior shoulder pain. Some patients may report locking of the shoulder in certain position.
Clinical examination of the shoulder may reveal shoulder instability. There is apprehension in the abduction and lateral rotation.
A crepitus may be noted on examination.
Imaging
X-rays are mostly without any specific findings. MRI is the modality of choice for assessment of HAGL.
The finding may be difficult to diagnose on arthroscopy. Typical findings include avulsion of the inferior glenohumeral ligament from the proximal humerus [ it must be stressed that the avulsion is more common at the glenoid (40%) or mid-substance (35%). Only 25% tearing occurs at the humerus
Retraction of the inferior glenohumeral ligament depicted by J sign. [The normal shape visible is U because the ligament droops down to give the appearance of a U] Disruption of this normality causes J sign.
As most of the HAGL lesions are associated with history of anterior shoulder dislocation, following signs are seen in 65% cases.
- Bankart lesion and/or anterior labrum injuries
- Subscapularis tear
- Hill-Sachs lesion
Treatment of HAGL
HAGL lesions respond poorly to conservative management and surgery is associated with better functional outcomes.
Surgical treatment includes open or arthroscopic repair of the avulsion. Both produce good results and functional outcomes appear to be good for patients undergoing either open or arthroscopic management.
The majority of patients show resolution of instability and pain cessation with surgical treatment of HAGL lesions.
References
- Bokor D, Conboy V, Olson C. Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament. J Bone Joint Surg Br. 1999;81:93–96.
- Bhatia DN, DasGupta B. Surgical treatment of significant glenoid bone defects and associated humeral avulsions of glenohumeral ligament (HAGL) lesions in anterior shoulder instability. Knee Surg Sports Traumatol Arthrosc. 2013;21(7):1603–1609.
- Bui-Mansfield LT, Banks KP, Taylor DC. Humeral avulsion of the glenohumeral ligaments the HAGL lesion. Am J Sports Med. 2007;35(11):1960–1966.
- Gehrmann RM, DeLuca PF, Bartolozzi AR. Humeral avulsion of the glenohumeral ligament caused by microtrauma to the anterior capsule in an overhand throwing athlete: a case report. Am J Sports Med. 2003;31(4):617–619.
- Oberlander MA, Morgan BE, Visotsky JL. The BHAGL lesion: a new variant of anterior shoulder instability. Arthroscopy. 1996;12(5):627–633.
- Wolf EM, Cheng JC, Dickson K. Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy. 1995;11(5):600–607.