Last Updated on November 22, 2023
High ankle sprains, also known as syndesmotic sprains, are sprains of the syndesmotic ligaments that connect distal ends of the tibia and fibula. High ankle sprains [because they are located above the ankle] comprise approximately 15% of all ankle sprains. These injuries are mostly external rotation injuries
Most of these occur in conjunction with ankle fractures and rarely in isolated form.
Relevant Anatomy
[Read anatomy of ankle joint]
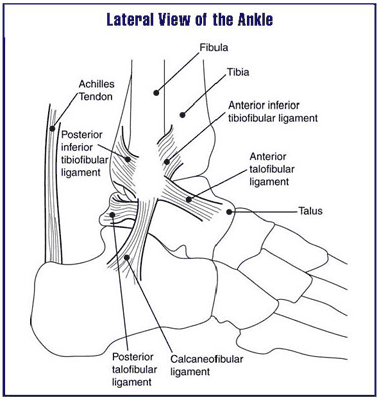
Syndesmosis is made up of
- Anterior-inferior tibiofibular ligament
- Originates from anterolateral tubercle of the tibia (Chaput’s)
- Inserts on anterior tubercle of the fibula (Wagstaffe’s)
- Posterior-inferior tibiofibular ligament
- Originates from posterior tubercle of the tibia (Volkmann’s)
- Inserts on the posterior part of the lateral malleolus
- Strongest component of a syndesmosis
- Inferior transverse tibiofibular ligaments
- Interosseous membrane
- Interosseous ligament
- Distal continuation of the interosseous membrane
- Main restraint to proximal migration of the talus
The main function of the syndesmosis maintains integrity between tibia and fibula. It resists axial, rotational, and translational forces. Deltoid ligament is the medial ligament that indirectly stabilizes the medial ankle mortise.
During normal gait, syndesmosis widens 1mm during gait
Following displacement is noted when these ligaments are sectioned.
- Anterior tibiofibular ligament – Diastasis of 2.3 mm
- Anterior tibiofibular ligament and interosseous ligament – Diastasis of 4.5 mm
- All 3 ligaments – 7.3 mm
Associated Injuries with High Ankle Sprains
- Osteochondral defects (15% to 25%)
- Peroneal tendon injuries (up to 25%)
- Ankle fractures
- Distal tibia and fibula
- 5th metatarsal base
- Anterior process of the calcaneus
- Lateral or posterior process of the talus
- Deltoid ligament injury
- Loose bodies
Pathophysiology
High ankle sprains are most commonly associated with external rotation injuries. External rotation forces the talus to rotate laterally and push the fibula away from tibia that may lead to
- Increased compressive stresses are seen by the tibia
- Increased risk of lateral subluxation of the distal fibula
- The incongruence of the ankle joint articulation
The most vulnerable structure is the anterior inferior tibiofibular ligament.
Different Injury Patterns
- Isolated Syndesmotic injury
- Syndesmotic injury & fibular fractures
- Syndesmotic injury + medial injury
- Syndesmotic injury+Posterior malleolus fracture
Clinical Presentation
There would be a pain on the anterolateral aspect of ankle proximal to the anteroinferior tibiofibular ligament. The ankle would be swollen and the patient is often able to bear the weight and walk [in contrast lateral ankle sprains are often able to bear weight]
The examination would reveal the tenderness of the syndesmosis.
Following provocative tests indicate high ankle sprain
Squeeze test
It consists of compression of tibia and fibula at midcalf resulting in pain at syndesmosis. If pain occurs, it is considered positive for syndesmotic injury.
External rotation stress test
Pain over syndesmosis is elicited with external rotation/dorsiflexion of the foot with knee and hip flexed to 90 degrees.
Cotton Test
Widening of the syndesmosis with lateral pull on the fibula
Fibular translation
Anterior and posterior drawer force to the fibula with the tibia stabilized causes increased translation of the fibula. There would be a pain with compression too (Patient dorsiflexes the foot while the examiner compresses the internal and external malleolus),
Imaging
X-rays
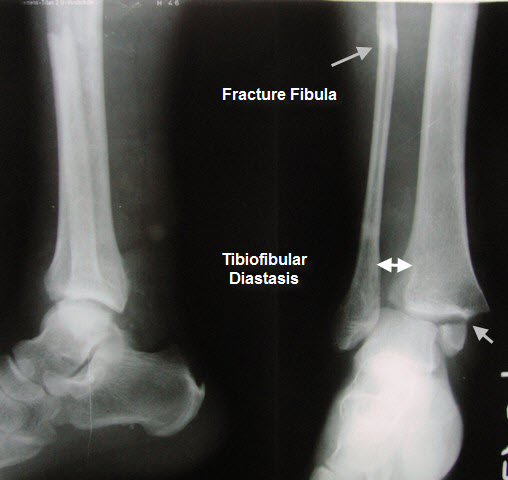
Recommended views are AP, lateral, mortise view of the ankle. AP and lateral views of the leg can be also done to rule out high fibula fracture.
Optional views include stress views in external rotation and gravity stress.
For comparison, opposite ankle x-rays can be done.
The AP view would show decreased tibiofibular overlap [normal>6mm]. The mortise view would also show decreased overlap [normal >1 mm]
There would be increased medial clear space [normal <4 mm] and increased tibiofibular clear space [normal <6 mm on both AP and mortise views]
CT
CT is more sensitive than x-rays and is indicated when the x-rays are normal and there is clinical suspicion of syndesmotic injury.
CT is also useful for postoperative assessment of reduction of syndesmosis after fixation
MRI
CT is also done when there is clinical suspicion of syndesmotic injury in the presence of normal x-rays. It is a very sensitive and specific investigation for detecting syndesmotic injury.
Treatment of High Ankle Sprains
Nonoperative Treatment
Non-operative treatment consists of controlled ankle motion [CAM] boot or cast for 2 to 3 weeks.
It is used in syndesmotic sprain without diastasis or ankle instability.
The weight bearing is delayed until the patient is pain-free. Following this physical therapy program is initiated. A brace that limits external rotation is used intermittently.
The recovery period is long and can take as much as twice that of standard ankle sprain
Operative Treatment
Indications for operative treatment are
- syndesmotic sprain without fracture with instability on stress radiographs
- Syndesmotic sprain refractory to conservative treatment
- Syndesmotic injury with an associated fracture that remains unstable after fixation of the fracture
Surgical Options
Syndesmosis screw fixation
- Two 3.5 or 4.5 mm syndesmotic screws that pass from fibula to tibia and engage at least one cortex of tibia.
- Conventionally, the ankle is held in maximum dorsiflexion to avoid overtightening
- The patient is kept non-weight-bearing for 6-12 weeks or longer
Syndesmosis Fixation with Suture Button
- Fiberwire suture with two buttons tensioned around the syndesmosis
- This can be done in addition to a screw
Prognosis
Missed injuries may result in degenerative ankle arthritis.
Anatomical reduction of syndesmosis results in an excellent outcome.