Last Updated on August 27, 2023
Spinal nerves are the nerves that originate in the spinal cord and form part of the peripheral nervous system.
Spinal nerves are mixed types of nerves. A mixed nerve is one which transmits motor, sensory, and autonomic signals between the spinal cord and the body.
In humans, there are 31 spinal nerves on each side of the vertebral column making it 31 pairs in total.
Types of Spinal Nerves
Depending on the region they originate from spinal nerves are called cervical nerves, thoracic nerves, lumbar nerves, sacral nerves, and coccygeal nerves.
Out of 31 pairs of spinal nerves, 8 are cervical nerves, 12 thoracic nerves, 5 lumbar nerves, 5 sacral nerves, and 1 coccygeal nerve.
Myotome refers to the muscles that one particular spinal root supplies and the dermatome are the area of skin supplied by a particular spinal nerve.
Structure of Spinal Nerves
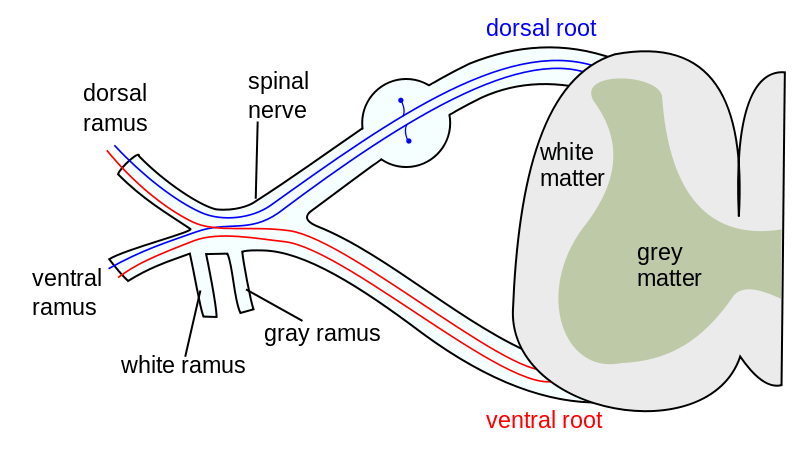
Each spinal nerve is formed by the combination of anterior and posterior roots for that particular spinal segment. The posterior or dorsal root is the sensory root of a spinal nerve and the anterior or ventral root is the motor nerve.
The spinal nerve emerges from the spinal column through intervertebral foramen between adjacent vertebrae except for C1 spinal nerve which emerges between the occipital bone and the first vertebra [atlas].
The first seven cervical nerves C1-C7 exit above the corresponding cervical vertebra but C8 cervical nerve exists below vertebra C7 and above vertebra T1. Rest of the spinal nerves [thoracic, lumbar, and sacral] an exit below the corresponding vertebra.
After it leaves vertebral column, spinal nerve divides into dorsal or posterior ramus, ventral or anterior ramus, and rami communicans, each carrying both sensory and motor information.
The posterior ramus or dorsal ramus is a smaller branch that supplies the posterior portions of the trunk and skin and muscles of the back except for first cervical, the fourth and fifth sacral, and the coccygeal.
The anterior ramus is a larger branch containing nerves that serve the remaining anterior parts of the trunk and the upper and lower limbs.
Except for the thoracic region where they remain distinct from each other and innervate a narrow strip of muscle and skin along the sides, chest, ribs, and abdominal wall as intercostal nerves, anterior rami form nerve plexuses by extensive branching and reuniting. Plexus results in redistribution of fibers from various rami and outgoing nerves from plexuses carry fires from different spinal nerves.
The cervical plexus is formed by anterior rami of spinal nerves C1-C4 and give out muscular branches to the neck, muscles of the neck, the diaphragm, and cutaneous branches to the skin of the neck and upper chest. The brachial plexus is formed by anterior rami from spinal nerves C5-T1 and supplies pectoral girdle and upper limb. The lumbar plexus is formed by anterior rami from spinal nerves L1-L4. The sacral plexus contains anterior rami from spinal nerves L4-S4. The lumbar and sacral plexuses supply the pelvic girdle and lower limbs.
The meningeal branches ( sinuvertebral nerves) are branches of spinal nerves that and re-enter the intervertebral foramen to supply the ligaments, dura, blood vessels, intervertebral discs, facet joints, and periosteum of the vertebrae.
The rami communicantes [or communicans] contain autonomic nerves carrying visceral motor and sensory information to and from the visceral organs.
Cervical Nerves
Cervical vertebrae are seven in number [C1-C7] and there are eight cervical nerves (C1-C8). C1-C7 cervical nerves emerge above their corresponding vertebrae but C8 nerve emerges below the C7. The posterior distribution of cervical nerves includes the suboccipital, greater occipital and third occipital. Anterior rami forms cervical plexus (C1-C4) and brachial plexus (C5-T1).
Thoracic Nerves
The thoracic nerves are 12 spinal nerves that exit the spine and go directly to the paravertebral ganglia of the autonomic nervous system where they are involved in the functions of organs and glands in the head, neck, thorax, and abdomen.
Anterior rami forms the intercostal nerves between T1-T12 that run beneath the corresponding rib. T2 and T3 nerves also branch to form the intercostobrachial nerve.
Posterior ramus form cutaneous and muscular branches to back in the thoracic region.
Lumbar Nerves
The lumbar nerves are the five spinal nerves emerging from the lumbar vertebrae.
Lumbar nerves are numbered by the vertebra above. If the first sacral vertebra is lumbarized (there are six lumbar vertebrae) or a sacralized L5 vertebra [four lumbar vertebrae, fifth is part of sacrum], the nerves are typically still counted to L5 and the next nerve is S1.
Posterior rami through their medial and lateral branches supply multifidus muscle and erector spinae muscles and skin on the lower back.
The first three anterior rami and part of fourth connect to form lumbar plexus. Part of fourth and fifth lumbar nerve forms a lumbosacral trunk, which takes part in the formation of the sacral plexus.
Sacral and Coccygeal Nerves
Sacral nerves are the five pairs of spinal nerves which exit the sacrum at the lower end of the vertebral column. The coccygeal nerve is the 31st spinal nerve.
The anterior divisions of the sacral and coccygeal nerves form the sacral and pudendal plexuses. The sacral plexus is formed by the lumbosacral trunk, the anterior division of the first, and portions of the anterior divisions of the second and third sacral nerves.
The pudendal plexus lies on the posterior wall of the pelvis and is not sharply demarcated from sacral plexus. It is usually formed by branches from the anterior divisions of the second and third sacral nerves, the whole of the anterior divisions of the fourth and fifth sacral nerves, and the coccygeal nerve.
The fifth sacral nerve receives a communicating filament from the fourth and unites with the coccygeal nerve to form the coccygeal plexus. From this plexus, the anococcygeal nerves take origin which pierces the sacrotuberous ligament to supply the skin in the region of the coccyx.