Last Updated on October 8, 2019
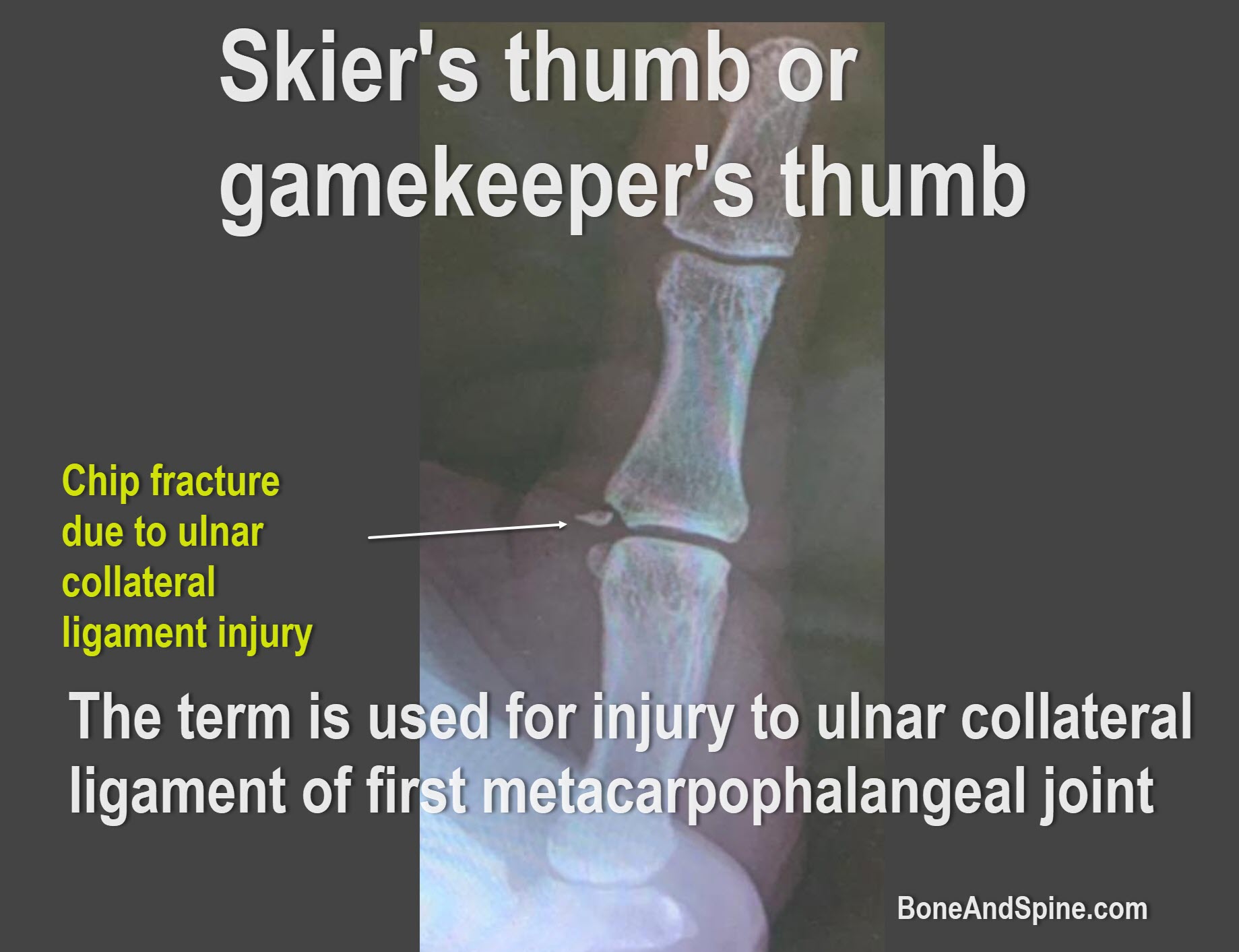
Terms Skier’s thumb and Gamekeeper’s thumb are used for injuries to the ulnar collateral ligament of first metacarpal joint. While Gamekeeper’s thumb was the older term, Skier’s thumb is used more commonly.
Ulnar collateral ligament injury of the metacarpal joint was found earlier in people of Europe who wrung the neck of the game like chicken, rabbits, between index finger and thumb. It leads to the stretching of the ligament resulting in instability of the metacarpophalangeal joint. That is why the condition was called the gamekeeper’s thumb.
However, today the acute trauma is the most common cause of the injury instead of chronic and repetitive. Because skiing accidents are most commonly responsible, the injury is known nowadays as Skier’s thumb.
Occasionally, the injury avulses the bone at its insertion and leads to a gamekeeper’s fracture or Skier’s fracture.
The injury of occurs when a skier’s hand lands on a ski pole, causing a valgus force on the thumb.
Skier’s thumb is the most frequent injury of the upper limb in skiers. There is no known sex predilection
Relevant Anatomy
Ulnar collateral ligament originates from the ulnar aspect of the metacarpal head and inserted distally on the ulnar aspect of the base proximal phalanx.
The metacarpophalngeal joint is a diarthrodial joint and mainly carries flexion and extension movements.
The joint stability is provided by the static and dynamic stabilizers.
Extrinsic and intrinsic hand muscles are the dynamic stabilizers especially adductor mechanism that also inserts on to the extensor expansion[The aponeurosis connecting the two is superficial to ulnar collateral ligament]
The static restraints include
- Collateral ligament (mostly in flexion)
- Accessory collateral ligament (mostly in extension)
- Palmar plate (mostly in extension)
- Dorsal capsule (limited, in flexion).
Normal variations of the joint movement at metacarpophlangeal joint are
- 5-115 degrees in flexion-extension plane
- Valgus laxity
- 6 degrees in extension
- 12-15 degrees in flexion
Mechanism of Injury
Acute abduction is the most common cause of ulnar collateral ligament.
A combination of torsion, abduction, and hyperextension at the first metacarpophalangeal joint may add to the injury.
The ligament may tear partially or completely
Most of the skier’s thumbs are injured due to fall on the ski poles which requires to strap and a sword-like grip formation. During fall this transmits the force to the thumb.
However, a simple fall on outstretched hand could lead to the injury too.
Other sports where the injury can occur are ball sports like football, basketball or those which use sticks like basketball or football.
Most tears occur distally, near the insertion of the ligament into the proximal phalanx, but canoccur proximally near the origin on the metacarpal head.
Stener lesion refers to the interposition of the adductor aponeurosis between the ruptured ulnar collateral ligaments and its site of insertion at the base of the proximal phalanx. This causes the distal portion of the ligament to retract and point superficially and proximally. It is felt as a lump.
It prevents the reduction of ulnar collateral ligament and the ligament cannot heal unless it is dealt surgically.
A rupture of the proper and accessory collateral ligaments must occur for this injury to happen.
Clinical Presentation
The patient complains of jamming of thumb and pain on the ulnar side of thumb following a fall, with ski pole or ball.
In case of chronic repeated injury, the patient reports of weakness in grasping or pinching ability. In case of complete tears, the patient is unable to perform these movements.
On examination, there could be swelling, discoloration and tenderness at the metacarpophalngeal joint. The severity of soft tissue changes often points to the severity of ligament damage.
Lump at the ulnar aspect of the metacarpophalangeal joint is indicative of a Stener lesion.
Pinch is markedly weakened.
Stress Testing
If the stress test is painful, examination can be performed under local anesthetic.
Stress testing is done by applying radially directed force on the metacarpophlangeal joint. The joint mobility in extension and 30 degrees flexion is compared with normal side.
A difference of more than 30 degrees compared to normal side is considered suggestive of rupture.
The test is positive in chronic instability also in spite minimal symptoms.
Classification of Skier’s Thumb
- Grade 1 – Sprain without instability of the metacarpophalangeal joint.
- Grade 2 – An incomplete tear with joint laxity.
- Grade 3 – A complete tear with instability of the joint.
Differential Diagnoses
Lab Studies
No lab tests are required for the diagnosis, but routine work up is needed for surgical intervention.
Imaging
Anteroposterior, lateral, and oblique x-rays are done to exclude metacarpal fractures and skier’s fractures.
X-rays should be performed before anymanipulation like stress test is done.
Following suggest instability
- Volar subluxation of 3 mm or more
- Instability is also indicated in cases in which there is a radial deviation of >40 degrees in extension and >20 degrees in flexion.
Stress radiographs [valgus stress] in flexion and extension to determine the degree of instability. A joint opening that is greater than 30º while the MCP is fully flexed is consistent with a complete rupture of the ulnar collateral ligament.
Sag Sign
The sag sign is a volar subluxation of the proximal phalanx relative to the metacarpal at the metacarpophalangeal joint, evident on plain film. In indicates UCL insuffiency.
MRI
MRI is useful but not always necessary and is not cost-effective. It outlines the details of the injury better.
Ultrasound
Ultrasonography can help differentiate between complete and incomplete tears.
Treatment of Skier’s Thumb
Grades 1 and 2 skier’s thumbs and incomplete UCL ruptures can be treated conservatively with proper immobilization. For small, nondisplaced avulsion fractures of the proximal phalanx that are found to be stable on stress testing, nonoperative treatment by a spica-type cast for 4 weeks can be completed with good results.
Nonoperative treatment can also be considered in patients that either refuse surgery or who are too infirm to tolerate an operative procedure
A 50% failure rate is reported with complete tears that are treated with bracing and early motion
Primary surgical repair is indicated for the following:
- Complete rupture of the UCL, as evidenced by joint instability
- UCL damage with any accompanying fracture that is displaced, rotated, or intra-articular
- Presence of a Stener lesion
To prevent chronic painful instability, weakness of pinch, and arthritis, surgical treatment is recommended for fractures with 2 mm or more of displacement, or significant articular involvement with incongruency or rotation.
Stener lesion results in permanent instability and is an indication for surgical repair.
Nonoperative treatment
This may be treated with immobilization in a thumb spica-type cast for 4 weeks. The metacarpophlangeal joint is left in 20° of flexion with mild ulnar deviation (adduction) to reduce stress on the ligament, and the interphalangeal joint is also placed in slight flexion.
After 4 weeks, active-range-of-motion exercises, stretching exercises and strengthening exercises can be used to help the return of strength and functioning.
Surgical Treatment
Complete ruptures of are repaired preferably in the first week or within three weeks as the repair of these lesions after 3 weeks has an increased incidence of weakness and pain on pinch grasp.
It could be just soft-tissue repair seems or aided by a small-gauge Kirschner wire to the metacarpophalangeal joint in position in case the soft tissue repair does not reduce the joint.
In the case of chronic instaity ligament reconstruction using a free tendon, usually the palmaris longus] is done.
If arthritis is present an arthrodesis of the metacarpophalangeal joint is considered.
After surgery, a volar plaster splint is used to immobilize the thumb and wrist for 4-5 weeks following the operation.
At 4 weeks, the cast and any pins that were placed may be removed. The patient is then placed in a hand-based splint that immobilizes the MCP joint for 2 weeks. The splint is removed for therapy during this 2-week period, and active motion of the MCP joint is begun. Unrestricted usage is allowed at 3 months.
Complications
- Radial sensory nerve injury
- Postsurgical stiffness of the MCP and interphalangeal joints to improve with time.
References
- Hung CY, Chang KV. Gamekeepers Thumb (Skiers, Ulnar Collateral Ligament Tear). 2018 Jan. 35(8):1321-5.
- Gerber C, Senn E, Matter P. Skier’s thumb. Surgical treatment of recent injuries to the ulnar collateral ligament of the thumb’s metacarpophalangeal joint. Am J Sports Med. 1981 May-Jun. 9(3):171-7.
- Heyman P. Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint. J Am Acad Orthop Surg. 1997 Jul. 5(4):224-9.
- Ritting AW, Baldwin PC, Rodner CM. Ulnar collateral ligament injury of the thumb metacarpophalangeal joint. Clin J Sport Med. 2010 Mar. 20(2):106-12.