Last Updated on May 24, 2022
Cervical spine clearance refers to the confirmation of the absence of cervical spine injury in a patient of trauma. It is part of the evaluation of a trauma patient. Cervical injuries are found in about 4 percent of blunt trauma patients.
All trauma patients are said to have cervical injury unless proven otherwise.
Therefore cervical spine clearance becomes essential. Cervical spine clearance or c-spine clearance can be done clinically and radiologically.
The frequent challenges that one faces in clinical evaluation are
- Altered mental status
- Head injury
- Intoxication
- Distracting injuries [injuries like long bone fracture, visceral injuries, etc]
- Patient’s inability to cooperate
It must also be emphasized here that in case the cervical spine injury is present, the entire spine should be examined for the injury as up to 15 percent of patients with cervical spine injuries have noncontiguous spine injuries.
Need for Cervical Spine Clearance
During the initial examination of the trauma patient, a cervical collar often is applied to restrict cervical spine motion. Clearance of the cervical spine allows removal of the collar early and in an efficient manner. Otherwise, unnecessary immobilization not only adds to the nursing care burden and patient inconvenience but also increases the likelihood of the complications associated with hard cervical collar usage.
Prolonged immobilization with a collar may increase the risk of
- Pressure ulcers [face or skull]
- Interference with airway and ventilation
- Infection
- Increase in intracranial pressure in cases of head injury
- Increased risk of aspirationMortality increased in geriatric patients
- Increase in mortality [elderly patients]
Moreover, it is crucial to identify patients who have an overt cervical injury or have cervical spine instability that could further damage the spinal cord.
If cervical spine clearance protocol is not applied, it leads to
- Inadequate assessment
- Missed injuries
- Complications of prolonged immobilization [when the cervical injury is not present]
- A complication of cervical injuries [when present]
Therefore, it Is important to identify promptly who does not require collar use and cervical care [and who does].
Cervical Spine Clearance in Adults
A cleared spine in a patient means that diligent spine evaluation is complete and the patient does not have a spinal injury requiring treatment.
All trauma patients are at risk for a spinal injury and systematic evaluation is necessary to achieve the goal of no missed injuries.
Two of the most common decision tools [set of guidelines] developed are
- National Emergency X-Radiography Utilization Study (NEXUS) Low-Risk Criteria
- Canadian C-Spine Rule
The Canadian C-Spine Rule is complex and requires a series of examinations. Canadian C-spine rule also had limitations of application in some patient groups like children and pregnant women.
The examination of the patient begins with receiving the patient at the accident site or in the hospital.
After general trauma examination [airway, breathing, circulation, and taking care of critical things first, visual and manual inspection of the entire spine is done. The following things are noted
- Degree of consciousness
- Any neurologic deficits
- Any known issue that could increase risk of spine injury [preexisting cervical fusion, ankylosing spondylitis, connective tissue disorders]
- Seat belt sign – may suggest spinal injury
For cervical spine examination
- Look for angular or rotational deformities of the neck
- Palpate for tenderness along the midline
- Absent tenderness in an awake patient almost rules out cervical injury
- Neurological examination
Cervical spine clearance begins with a set of questions or observations
- Mechanism of injury [is it likely to result in a cervical injury]
- Fall from more than 10 feet in height
- Motor vehicle accidents at a speed greater than 55 miles per hour
- Likely hyperextension injury –
- Patient falls and hits forehead
- Rear-end collision
- Neck pain or tenderness
- Any neural deficit
- Age more than 65 years
- Obtunded patient
- Altered mental status
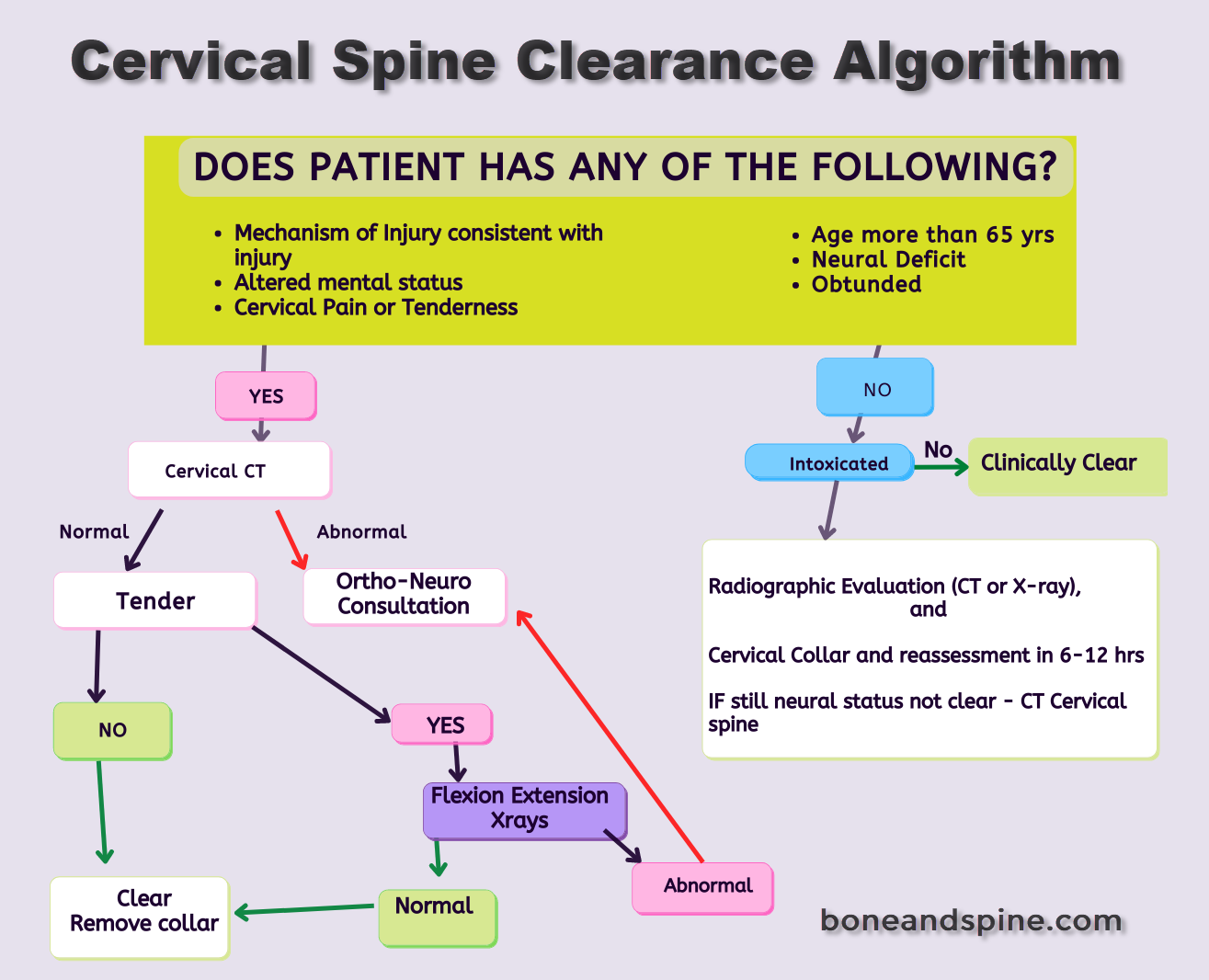
If the answer is no
If the answer to all the questions is NO, and the patient is not intoxicated, the cervical spine is clear.
If the answer is No and the patient is intoxicated, the patient is put on a cervical collar and x-rays [or CT in some cases] are done. The patient is reassessed after 6-12 hours. If still not clear – CT cervical spine is done. Further examination is dependent on the alertness level of the patient.
An abnormal CT warrants neurosurgery and orthopedics examination of the patient.
If the answer is yes
A cervical CT of the patient is done. Those with abnormal CT require ortho/neuro evaluation.
A patient with normal CT is examined for neck tenderness. IF not tender, the cervical spine is clear.
If the neck is tender, flexion-extension x-rays can be obtained to look for cervical instability. Abnormal x-rays warrant ortho/neuro opinion.
Thus, clinical examination is the mainstay of cervical spine clearance in patients who are alert [not intoxicated or have distracting injury]
In the case of obtunded patients, the collar should be removed only after CT shows no injury.
cervical collars could be removed from obtunded patients only after a negative high-quality CT of the cervical spine alone failed to detect an injury
many authors have questioned the efficacy of flexion-extension x-rays as these are expensive and often not effective.
MRI can detect many injuries that CT does not because of its high sensitivity but does not add any benefit to evaluation. That means CT is able to detect functionally significant injuries.
Cervical spine injury should be considered in an unconscious patient even in the absence of a definitive history of trauma.
Workable summary of the cervical spine clearance in adults
Cervical clearance can be given clinically if the
- The patient is awake, and not intoxicated
- No distracting injuries
- No neck pain or tenderness
- No neurological deficit
Radiological spine clearance is required when
- Obtunded or intoxicated patient
- Neck pain or tenderness
- Presence of distracting injury
- Imaging done
- X-rays – AP, lateral and open mouth view
- CT
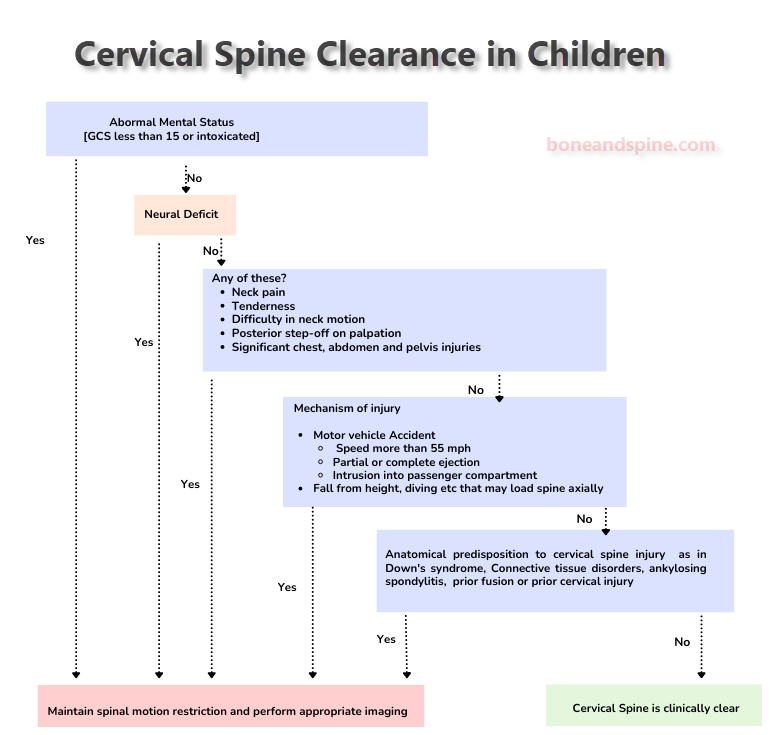
Cervical Spine Clearance in Children
Clinical cervical spine clearance can be given in communicating with patients older than 3 years when
- Mental status is normal
- No change in alertness level
- Absence of tenderness of cervical spine/neck soft tissues
- No neurological deficit
- Absence of distracting injuries
- Painfree neck movements
In this scenario, x-rays may not be done and the cervical collar is removed.
–All other patients which do not fit the above criteria are considered for CT cervical spine.
–Any abnormal clinical/ radiological warrants specialist consultation and cervical spine immobilization is continued.
–Those patients whose spine is not cleared within two hours [either delay or warranting consultation from specialist], a pediatric collar should be applied after removing the extrication collar as they are often wrong sized for kids.
All those patients with abnormal clinical findings and those with the status that hinders examination MRI should be sought. Flexion-extension x-rays can be done if MRI is not possible. These are done to look for cervical spine instability.
In children with preexisting conditions causing cervical instability such as collagen diseases, trisomy of 18 etc], the examination is not considered reliable and consultation should be sought.
References
- Halpern CH, Milby AH, Guo W, et al. Clearance of the cervical spine in clinically unevaluable trauma patients. Spine. 2010;35(18):1721–1728. [Link]
- Menaker J, Philp A, Boswell S, Scalea TM. Computed tomography alone for cervical spine clearance in the unreliable patient—are we there yet. J Trauma. 2008;64(4):898–904.
- Sim V, Bernstein MP, Frangos SG, et al. The (f)utility of flexion-extension C-spine films in the setting of trauma. Am J Surg. 2013;206(6):929–934.
- Tran B, Saxe JM, Ekeh AP. Are flexion-extension films necessary for cervical spine clearance in patients with neck pain after negative cervical CT scan. J Surg Res. 2013;184(1):411–413.
- Trauma Association of Canada Pediatric Subcommittee National Pediatric Cervical Spine Evaluation Pathway: Consensus Guidelines. Journal of Trauma, 2011;70: 873-884
- Lee, S., Sena, M., Greenholz, S., & Fledderman, M. (2003). A Multidisciplinary approach to the development of a cervical spine clearance protocol: Process, rationale, and initial results. Journal of Pediatric Surgery, 38(3), 358-362