Last Updated on October 28, 2023
The dorsal scapular nerve entrapment is a relatively less common nerve entrapment that causes shoulder and arm pain. It is vulnerable during brachial plexus injections as the nerve passes through the middle scalene muscle.
Dorsal scapular nerve entrapment is uncommon and therefore frequently underrecognized cause of pain in shoulder and neck area.
The symptoms are easily mistaken for other problems.
Relevant Anatomy
Anatomy of Dorsal Scapular Nerve
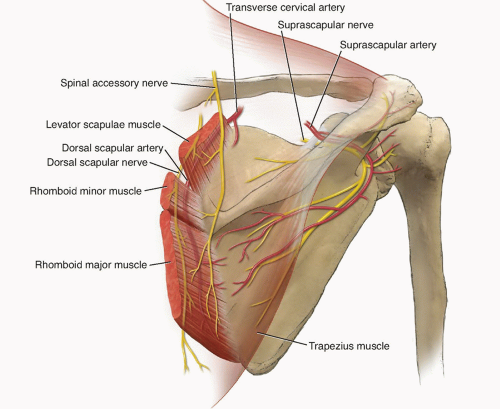
The dorsal scapular nerve arises from the brachial plexus, usually from the cervical nerve C5. After leaving C5, it commonly pierces the middle scalene muscle and continues beneath the undersurface of levator scapulae and the rhomboids.
It provides motor innervation to the rhomboid muscles, which pull the scapula towards the spine and levator scapulae muscle, which elevates the scapula.
The course of the nerve is accompanied by one of two arteries: either the dorsal scapular artery that arises from the third part of the subclavian artery or deep branch of the transverse cervical artery [when the other artery is absent].
It is a branch of the thyrocervical trunk which is a branch of the first part of the subclavian artery,
The dorsal scapular nerve supplies the levator scapulae muscles, the rhomboid major and minor muscles.
The rhomboids minor and major muscles connect the medial edge of the scapula to the spinal column. Both rhomboid muscles pull the scapula towards the midline (scapular adduction) and they also pull the scapula superiorly with downward rotation, function opposite to serratus anterior.
Anatomy of Rhomboids and Levator Scapulae
Rhomboids

There are two rhomboids are two muscles – rhomboid major & rhomboid minor.
Rhomboid major originates from spinous Processes T2-T5 and inserted on to medial border of scapula from level of the spine to inferior angle
Rhomboid Minor originates from nuchal ligament and spinous Processes C7 & T1. It inserts on a triangular area of the medial end of the medial end of the scapular spine
Both the rhomboids lie deep to trapezius and form parallel bands that pass inferolaterally from the vertebrae to the medial border of the scapula. The two are often separated by a small space between but in some cases, one single blended muscle may be present.
Levator Scapulae
It originates from the posterior tubercle of the first four transverse processes of cervical vertebrae and is inserted into medial border of the scapula extending from superior angle to junction of the spine and medial border of the scapula.
Causes of Dorsal Scapular Nerve Entrapment
- Entrapment in scalenus medius muscle
- Direct injury to the nerve
- Severe C5 root lesion or avulsion.[Brachial plexus injuries]
- Anterior shoulder dislocation
- C5 radiculopathy has also been suggested as a causative factor.
[In overhead athletics, a muscle injury to rhomboids may cause rhomboids palsy leading to winging of the scapula and mimicking dorsal scapular nerve entrapement]
Clinical Presentation and Diagnosis
Injury/entrapment of dorsal scapular nerve causes weakness of the levator scapulae and the rhomboid muscles and results in a winging of the scapula.
[Scapular winging refers to the abnormal protrusion of scapula on patients back. It occurs because of paralysis of stabilizing muscles of the scapula. Serratus anterior and trapezius are common causes whereas rhomboids weakness is an uncommon cause.
The scapular winging in dorsal scapular nerve syndrome is not as severe as seen with serratus anterior muscle and trapezius.]
The usual complaint in dorsal scapular nerve entrapment is a history of the abnormal movement of the shoulder joint, and stiff joint. The patient may also complain of pain in the shoulder region.
On examination, as noted before, there could be scapular winging. The scapula may become laterally displaced with an upward motion.
When asked to bring the scapulae together [adduct], the patient is not able to do so or the affected side is less adducted. Palpation of the contracted rhomboideus muscles would confirm the weakness.
When the patient is asked to move the arm forward on elevation will result in the medial border of the scapula being lifted and pulling on the inferior angle of this bone.
An electromyogram would help in confirmation of diagnosis.
MRI scan helps to diagnose roots avulsions.
Treatment of Dorsal Scapular Nerve Entrapment
Treatment usually is conservative which includes
- Cervical stabilization
- Cervical collar
- Cervical traction
- Muscle relaxants
- NSAIDs
- Physical therapy
- Strengthening of the trapezius [middle trapezius provides compensation for loss of rhomboids]
- Local steroid block for muscle
Surgery can be considered in severe cases that are unresponsive to conservative treatment.
The procedures are
- Fascial sling operation
- Two fascia lata grafts are used to connect the lower medial border of the scapula to the spinal muscles and the inferior angle of the scapula to the latissimus dorsi.
- This anchors the scapula to the posterior thoracic wall, eliminating winging.
- Grafts may stretch or fail with time
- Neurolysis or nerve decompression
- Suggested as last resort
References
- Tubbs RS, Tyler-Kabara EC, Aikens AC, Martin JP, Weed LL, Salter EG, Oakes W. Surgical anatomy of the dorsal scapular nerve. J Neurosurg. 2005 May; 102(5):910-1.
- Fisher MA, Gorelick PB. Entrapment neuropathies. Differential diagnosis and management. Postgrad Med. 1985 Jan; 77(1):160-74.
- Jerosch J, Castro WH, Geske B, Damage of the long thoracic and dorsal scapular nerve after traumatic shoulder dislocation: case report and review of the literature.Acta Orthop Belg. 1990; 56(3-4):625-7.