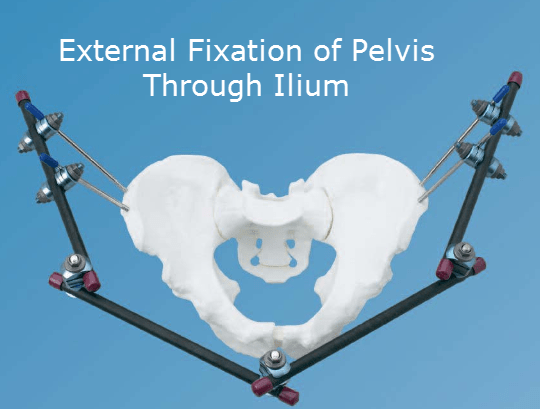
Last Updated on November 11, 2019
External fixation of pelvis is indicated for temporary or definitive stabilization of unstable pelvic ring injuries.
Temporary external fixator applied to a fractured pelvis can reduce internal hemorrhage dramatically and literally save someone’s life who is at risk from loss of blood.
Advantage of External Fixation of Pelvis
Pelvis bleeding after fracture of the pelvic ring is caused largely by tearing of pelvis veins which continue to bleed under low pressure until the lost blood fills the space it is in. only when the pressure of extravasated blood equals the venous pressure will bleeding stop. This could and often is only when the patient bleeds to death.
This procedure provides counter pressure or tamponade which stops venous bleeding.
Pelvic fixator may be applied quickly under local anesthesia through small skin puncture wounds and only takes a few minutes. Always take care not to compromise later surgery when placing the Schanz screws and as soon as the patient is hemodynamically stable check the pin position. The fracture will require more accurate investigation with CT scanning and may require internal fixation when it is safe to do so.
It is important to remember that external fixation (whether supra acetabular or iliac crest) predominantly controls and stabilizes the anterior pelvic ring. In most cases, supplemental stabilization or fixation is required for associated posterior pelvic ring injuries.
It could be difficult to apply this to obese patients.
It could also lead to definitive stabilization of some fractures such as rotationally unstable but vertically stable injuries.
The procedure is relatively contraindicated in the case of iliac wing fractures.
Procedure of External Fixation of Pelvis
Preoperative assessment x-rays must be done. These include an inlet, outlet, & AP views of pelvis. A CT is desirable but may be postponed because the patient needs urgent stabilization.
Intra-operative fluoroscopy is helpful and guides pin placement and reduction. But it may not be available at all centers.
Positioning and Draping
The patient is placed supine [flouroscopy table is if available]. The area from approx 5 cm above umbilicus to groin is prepped and draped. It includes bilateral flanks [ilium].
A large bean bag perpendicular to the patient’s torso helps to stabilize the patient.
It is important that the pelvis is manually reduced as much as possible prior to pin insertion.
If pelvis is unstable with vertical migration or posterior displacement, then traction is used through supracondylar femoral pin insertion.
Compression force can also be provided by tying a large towel around the pelvis.
Pins and Frames
Schanz pins should be at least 5 mm in diameter. Smaller pelves as in children require 4-mm pins.
Pins used should be of adequate length, to allow for postoperative swelling and the need for anteriorization of the frame.
Frame construct should be planned beforehand. A double frame construct allows for postoperative manipulation of one frame without losing the reduction.
A frame too close to the abdomen may cause impingement if abdominal distention occurs.
Pin Insertion
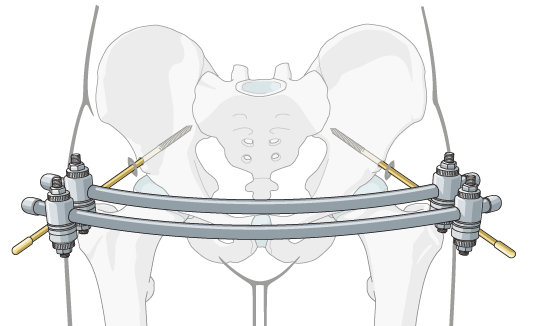
When pins are placed along the iliac wing, the number may vary from two to three. In case of the alternative method [described below], a single pin may suffice.
The first pin is usually placed about 2 cm posterior to anterosuperior spine. The rest of pins should then be placed along iliac crest using an external fixation clamp to determine the proper pin spacing.
A small incision on the iliac crest allows to find the appropriate orientation of wing and prevent skin tension on pins;
Pins are preferably placed in the outer half of the iliac crest in order to avoid cortical perforation and directed toward the acetabulum so that the pins are angled toward the patient’s head.
Cranially directed pins may cause be an impingement on the patient’s abdomen when sitting.
If C-arm image intensifier is available, pin placement can be confirmed at the time of insertion by using fluoroscopy.
Alternative Method
This method inserts pins distal to anterior superior iliac spine and anterior inferior iliac spine.
It is preferably done underfluoroscopic guidance.
Commercially Available External Fixators for Pelvis
There are many commercially available pelvic fixation devices available like C-clamp or Orthofix devices. These devices have advantages of quicker application and readiness.
After Care of External Fixation of Pelvis
Depending on the position, the patient might require intensive resuscitation efforts till stabilization. If internal fixation is contemplated, the fixator is kept only temporarily.
In some patients though, the fixator might serve as definitive treatment and is kept for about 12 weeks. When it is removed, the pelvis should be examined under fluoroscopy to make sure it is stable.
Depending on the fracture configuration, the weight-bearing may be allowed with the fixator in situ.
Weight-bearing is generally allowed if posterior stability is present. In case there is posterior instability, weight-bearing is not allowed through the patient is allowed to sit.
Complications of External Fixation of Pelvis
- Pin tract infection
- Loosening of pins
- Injury to the lateral cutaneous nerve
- Pressure Sores
- Bladder incarceration may result from the reduction of pubic symphysis diastasis especially when the bladder is herniated.