Last Updated on October 27, 2023
The leg has two bones – tibia and fibula. The fibula is very thin bone compared to the tibia and can be expended except for small length distally. This makes it usable for various orthopedic procedures. The fibula is homologous with the ulna. The fibula is a located on the lateral side of the tibia, with which it is connected above and below. The fibula is the slenderest of all the long bones.
Out of two bones, the tibia is called shin bone whereas fibula is called calf bone.
Structure of Fibula
The fibula has an upper end, shaft, and a lower end.
Upper End of Fibula
The upper end is slightly expanded in all directions making an irregular quadrate form. Its superior surface bears a circular articular facet directed upward, forward, and medialward, for articulation with a corresponding surface on the lateral condyle of the tibia.
On the lateral side is a thick and rough prominence continued behind into a pointed eminence, the apex or styloid process, which projects upward from the posterior part of the head.
Immediately below the head, the fibula constricts and the part is referred to as neck of the fibula.
Immediately below the head, the fibula constricts and the part is referred to as neck of the fibula.
Shaft of Fibula
The shaft of the fibula is slim and its shape is molded by attached muscles and therefore shows considerable variation in its form.
It has three borders
-anterior, posterior and interosseus
and three surface
– medial, lateral and posterior
Borders of the Shaft of Fibula
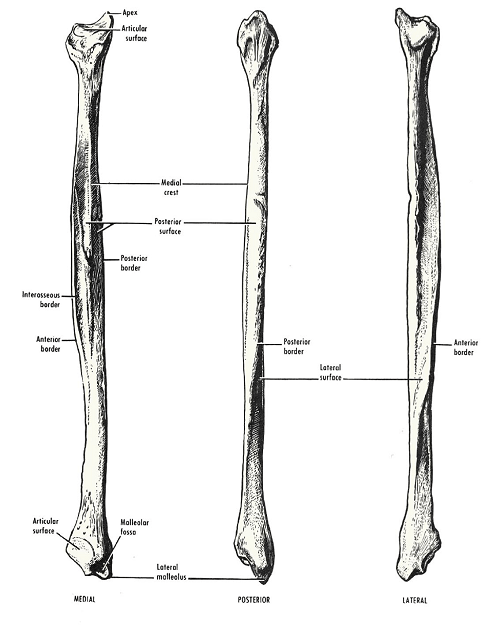
The Anterior Border
It begins just below the anterior aspect of the head. At the lower end, it divides to enclose an elongated triangular area which is continuous with the lateral surface of the lateral malleolus.
The Posterior Border
It is rounded and its upper end is in line with the styloid process. Below, the border is continuous with the medial margin of the groove on the back of the lateral malleolus.
Interosseus or Medial Border
It lies just medial to the anterior border, but on a more posterior plane. It ends below at the upper end of a roughened area above the talar facet of the lateral malleolus. In its upper two thirds, the interosseous border lies very close to the anterior border and may be indistinguishable from it.
Surfaces of Fibula
The medial surface
It lies between the anterior and interosseus borders. In its upper two thirds, it is very narrow, measuring 1 mm or less.
The lateral surface
It lies between the anterior and posterior borders. It is twisted backward in its lower part.
The posterior surface
It is the largest of the three surfaces. It lies between the interosseus and posterior borders. In its upper two thirds, it is divided into two parts by a vertical ridge called the medial crest.
Lower End of Fibula

It is also called lateral malleolus and along with the inferior surface of the tibia and medial malleolus participates information of ankle joint.
The tip of the lateral malleolus is 0.5 cm lower than that of the medial malleolus, and its anterior surface is 1.5 cm posterior to that of the medial malleolus. It has the following four surfaces.
The anterior surface is rough and rounded. The posterior surface is marked by a groove. The lateral surface is subcutaneous. The medial surface bears a triangular articular facet for the talus (anteriorly); and the malleolar fossa (posteriorly).
Attachments of Fibula Bone
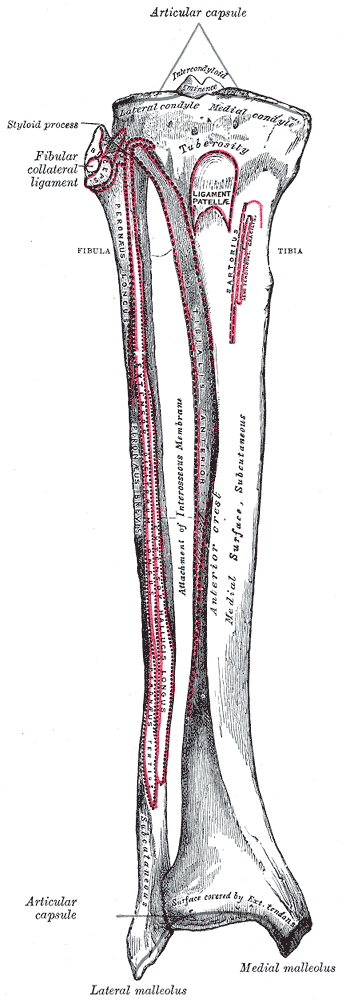
Head of Fibula
- C shaped insertion of the biceps femoris on the anterolateral slope of the apex.
- The fibular collateral ligament of the knee joint
- Extensions of origins of
- the extensor digitorum
- the peroneus longus
- the peroneus longus
- the soleus
- The capsular ligament of the superior tibio fibular joint – Around the articular facet.
Medial Surface of Fibula
- Origin of the
- Extensor digitorum longus- from the whole of the upper one fourth, and from the anterior half of the middle two fourths.
- Extensor hallucis longus – From the posterior half of its middle two-fourths
- Peroneus tertius (from its lower one fourth).
Lateral Surface of Fibula
- Origin of
- The peroneus longus (from its upper one third, and the posterior half of the middle one third
- The peroneus brevis (from the anterior half of its middle one third, and the whole of the lower one third)
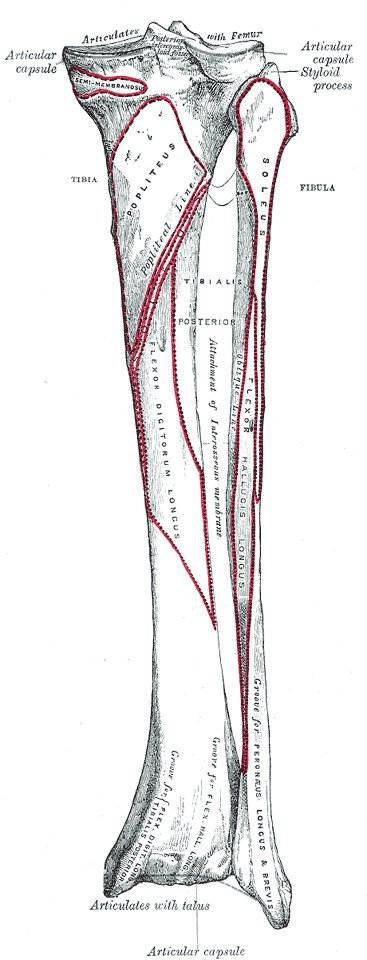
Posterior Surface of Fibula
- Tibialis Posterior – The part of the posterior surface between the medial crest and the interosseus border
- Soleus – Upper one-fourth of the part of the posterior surface between the medial crest and the posterior border
- Flexor hallucis longus – Lower three-fourths of the part of the posterior surface between the medial crest and the posterior border
Anterior Border
The anterior border of the fibula gives attachment to:
- The anterior intermuscular septum
- The superior extensor retinaculum (to the lower part of the anterior margin of the triangular area)
- The superior peroneal retinaculum (to the lower part of the posterior margin of the triangular area).
Posterior Border
- Posterior intermuscular septum.
- The triangular area above the medial surface of the lateral malleolus
- Anterior tibiofibular ligament (anteriorly)
- Interosseus tibiofibular ligament (in the middle)
- Posterior tibifibular ligament (posteriorly).
Interosseus border
- Interosseus membrane. The attachment leaves a gap at the upper end for passage of the anterior tibial vessels.
- Deep transverse fascial septum at the medial crest.
Lateral Malleolus
- Anterior talofibular ligament to the anterior surface.
- Inferior transverse tibiofibular ligament (above) and posterior tibiofibular ligament (below) to the malleolar fossa.
- The capsule of the ankle joint along the edges of the malleolar articular surface.
- The groove on the posterior surface of the malleolus lodges the tendon of the peroneus brevis and of the peroneus longus. Longus is superficial and brevis is deep.
Blood Supply
The peroneal artery gives off the nutrient artery for the fibula, which enters the bone on its posterior surface.
Ossification of Fibula
- One primary and two secondary centers.
- The primary center – for the shaft, appears during the 8th week of intrauterine life.
- A secondary center
- for the lower end appears during the first year and fuses with the shaft by 15-17 years.
- for the upper end appears during the 4th year, and fuses with the shaft by 17-19 years.
The fibula is unique because it is an exception to the law of ossification. Its secondary center which appears first also fuses first. But according to the law of ossification, the center that appears first would fuse last.
Clinical Significance
The fibula is a common bone to be fractured in ankle fractures and it is very important to restore normal fibular anatomy in ankle fractures with low fibula fractures.
The common peroneal nerve can be rolled against the neck of the fibula. This is an important landmark in clinical examination of nerve.
The fibula is an ideal spare bone for a bone graft and is commonly used in replacing the length of the bone or serve as to increase graft measure in various bone surgeries.
The lateral malleolus and the ligaments attached to it are very important in maintaining stability at the ankle joint.
Side Determination of Fibula
- The upper end, or head, is slightly expanded in all directions. The lower end or lateral malleolus is expanded anteroposteriorly and is flattened from side to side
- The medial side of the lower end bears a triangular articular facet anteriorly, and a deep fossa posteriorly.