Last Updated on August 1, 2019
Iliopsoas bursitis is an uncommon cause of anterior hip pain and is due to inflammation of iliopsoas bursa or iliopectineal bursa. Because of the rarity of occurrence and nonspecific presentation, the diagnosis of iliopsoas bursitis is may be overlooked.
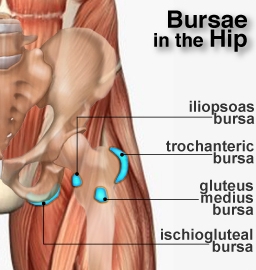
Relevant Anatomy
The iliopsoas bursa or iliopectineal bursa is the largest one in the body. It is located between the iliofemoral ligament of the hip and the iliopsoas tendon extending from lesser trochanter to the iliac fossa, underneath the iliac muscle. This bursa is present bilaterally in about 98% of the adults. 10-15% of the patients have a defect in the anterior part of the capsule of the hip, allowing the communication of the articular cavity with the bursa.
When healthy, the bursa is always collapsed. In 13% of all cases, the iliopectineal bursa is partly separated by a septum into two cavities, allowing tendon of the psoas major muscle to pass over the medial chamber and that of iliacus muscle over the lateral.
The psoas and iliacus muscles originate from the lumbar spine and pelvis and converge to form the iliopsoas muscle, which inserts onto the lesser trochanter. The iliopsoas muscle passes anterior to the pelvic brim and hip capsule in a groove between the anterior inferior iliac spine laterally and iliopectineal eminence medially.
The iliopsoas muscle acts as hip flexor and external rotator of the femur.
Causes of Iliopsoas Bursitis
- Rheumatoid arthritis
- Acute trauma
- Osteoarthritis
- Total hip arthroplasty,
- overuse injury
- Pigmented villonodular synovitis
- Osteochondromatosis
- Infection
- Crystal deposition disease
In sports activities, a bursitis is likely the result of repeated microtrauma caused by vigorous hip flexion and extension. Iliopsoas bursitis is commonly seen in individuals participating in strength training, rowing, uphill running etc.
Pathophysiology
It is theorized that when the hip is in flexion, both the iliopsoas muscle and the anterior part of the bursa move away from the hip joint. If the hip is to be hyperextended suddenly, there is a great tension that stretches the muscle and the bursa leading to bursal trauma.
According to another theory, when a flexed, abducted and externally rotated hip is brought into an extension, it causes an interruption of the lateral to medial movement of the iliopsoas tendon. Resulting in a painful snapping of the tendon over the anterior hip capsule.
A communication between this bursa and the hip joint is present in about 15% of healthy adults.
Presentation of Iliopsoas Bursitis [Signs and Symptoms]
The typical presentation of a patient with iliopsoas bursitis is a pain on the anterior aspect of the hip which gets worsened by activity such as walking or crossing the legs. Rest relieves the pain. A mass may or may not be felt. Morning stiffness and pain may be reported.
The pain may refer to abdomen, thigh or knee. The patient may inadvertently keep the limb in flexion, adduction and external rotation to decrease the tension in iliopsoas.
On examination, pain and tenderness may be localized at the midpoint of the inguinal ligament in femoral triangle. Bursitis can be palpated as a mass in the groin region.
The pain may be exacerbated by
- Hip extension
- Hip flexion resisted as well as passive
- Internal rotation
- adduction with the hip in flexion
A palpable or audible snap in the hip region may also be felt on examination.
To produce snap, the affected hip is extended from a position of flexion, abduction and external rotation.
Differential Diagnoses
- Snapping hip syndrome
- Trochanteric bursitis
- Radiculopathy
- Inguinal hernia
- Undescended testes
- Femoral artery aneurysm.
Imaging
Xrays
Xrays may be normal or show an underlying problem of the hip, such as osteoarthritis and rheumatoid arthritis.
USG
Ultrasound is a quick method to measure the size and the impact on surrounding structures.
MRI
MRI is the most accurate in detecting the size and is considered the imaging modality of choice in iliopsoas bursitis. It is able to distinguish the iliopsoas bursitis from other possible problems such as a tumor, hernia, hematoma, and aneurysm.
Treatment of Iliopsoas Bursitis
The treatment of iliopsoas bursitis is individualized for each patient according to the cause, pain severity and associated symptoms.
- Rest and avoidance of exacerbating activities
- Oral NSAIDs for pain and inflammation
- US-guided aspiration and injection of corticosteroids and anesthetic into the bursa
- Physical therapy
- Stretch exercise for hip
- Strengthening exercises for the hip rotators, hip flexors
- Quadriceps and hamstrings strengthening exercises
- Gait retraining to maintain hip stability
- Strengthening exercises of the abdominal muscles
- Surgery in refractory cases
- Removal of bursa [bursectomy]
- Capsulectomy
- Synovectomy possibly with iliopsoas tendon release.
Complications of Iliopsoas Bursitis
- Venous obstruction due to compression by the bursa
- Femoral neuropathy
- Compression of abdominal organs
- Rupture
- Infection