Last Updated on November 22, 2023
The knee joint is a modified hinge joint (ginglymus). The knee joint is not a very stable joint. Knee range of motion is through following movements-
- Flexion
- Extension
- Medial rotation
- Lateral rotation
The femur and lateral meniscus move over the tibia during rotation, while the femur rolls and glides over both menisci during extension-flexion. Thus the flexion-extension movement occurs in the compartment above the menisci whereas the rotator movement occurs below the menisci.
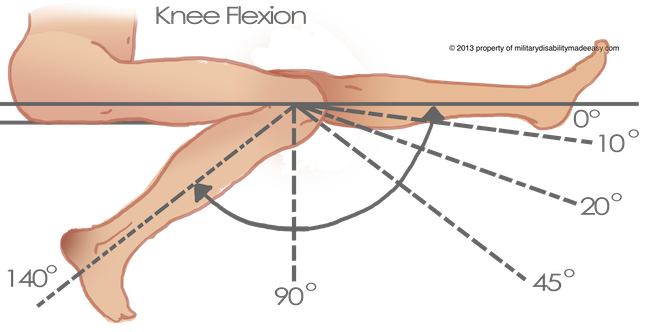
Normal Knee – Range of Motion
Normal range of motion of knee is
- Flexion – 120-150 degrees
- Internal rotation with knee flexed – 10 degrees
- External rotation with knee flexed – 30-40 degrees
The total range of motion is dependent on several parameters such as soft-tissue restraints, active insufficiency, and hamstring tightness.
Flexion-Extension Movement of Knee
Flexion and extension are the chief movements. These take place in the upper compartment of the joint, above the menisci.
They differ from the ordinary hinge movements in two ways
- The transverse axis around which these movements take place is not fixed. During extension, the axis moves forwards and upwards, and in the reverse direction during flexion. The distance between the center and the articular surfaces of the femur changes dynamically with the decreasing curvature of the femoral condyles.
- These movements are invariably accompanied by rotations (conjunct rotation). Medial rotation of the femur occurs during the last 30 degrees of extension and lateral rotation of the femur occurs during the initial stages of flexion when the foot is on the ground. When the foot is off the ground, the tibia rotates instead of the femur, in the opposite direction.
Rotatory Movements of Knee
Rotatory Movements at the knee are of a small range. Rotations take place around a vertical axis, and are permitted in the lower compartment of the joint, below the menisci.
Rotatory movements may be combined with flexion and extension (conjunct rotations) or may occur independently in a partially flexed knee (adjunct rotation).
In the flexed position, the collateral ligaments are relaxed while the cruciate ligaments are taut. Rotation is controlled by the twisted cruciate ligaments
The conjunct rotations are of value in locking and unlocking of the knee.
Passive Movements of Knee
Passive movements can be performed in a partially flexed knee. There is a lack of conformity between bony surfaces that allows translating movements in three planes.
This movement includes
- A wider range of rotation
- Anteroposterior gliding of the tibia on the femur
- Some adduction
- Some separation of the tibia from the femur.
Locking and Unlocking of the knee joint
Locking is a mechanism that allows the knee to remain in the position of full extension without much muscular effort. Locking occurs as a result of medial rotation of the femur during the last stage of extension.
As compared to the medial femoral condyle, the articular surface of the smaller lateral femoral condyle is a rounder and flattens more rapidly anteriorly. As a result when the lateral condylar articular surface if fully used up by extension, part of the medial condylar surface remains unused.
Lateral condyle of the femur attains a congruent relationship with its opposed tibial meniscal surface, about 30° before full extension has been obtained. To achieve full extension, the lagging medial compartment must medially rotate about a fixed vertical axis while moving backwards in an arc.
The lateral condylar servers as an axis around which the medial condyle rotates backwards [medial rotation of the femur] so that the remaining part of the medial condylar surface is also taken up. This locks the knee joint.
Locking is aided by the oblique pull of ligaments during the last stages of extension. When the knee is locked, it is completely rigid and all ligament of the joint are taut. Locking is produced by the continued action of the same muscles that produce extension i.e., the quadricps muscle.
The locked knee joint can be flexed only after it unlocked by a reversal of the medial rotation i.e., by lateral rotation of the femur. Unlocking is brought about by the action of the popliteus muscle and meniscal attachments.
It pulls downwards and posterior on its attachment to the lateral condyle of the and via its meniscal attachment the popliteus pulls on the posterior horn of the lateral meniscus.
Thus, while rolling back, the posterior motion of the menisci occurs in both compartments, but lateral more than medial.
Flexion and Extension Movements of Knee in Detail
This example considers foot fixed to the ground as in walking.
When the foot is fixed to the ground, the last 30° of extension is associated with medial rotation of the femur as explained above.
As the knee goes into extension, there is a progressive increase in the passive mechanism that resists further extension. In full extension following structures are tight and resist further extension
- Parts of both cruciate ligaments
- Collateral Ligaments
- Posterior capsule
- Oblique posterior ligament complex
- Skin and fascia
Moreover, there is also passive or active tension in the hamstrings, gastrocnemius muscles and the iliotibial band. Also, the anterior parts of the menisci compress between the femoral condyles and the tibia.
At the beginning of flexion, the knee unlocks by an external rotation of the femur on the tibia brought about by the opposite interplay of the meniscal articular and ligamentous structures and the contraction of the popliteus muscles.
Flexion is checked by the quadriceps mechanism, the anterior parts of the capsule and the PCL and by the compression of the soft tissue structures in the popliteal fossa.
Muscles Involved in Knee Movement
| Extension 5-10° | Flexion 120-150° |
| Quadriceps
Tensor fasciae latae [minor contribution] |
Semimembranosus Semitendinosus Biceps femoris Gracilis Sartorius Popliteus Gastrocnemius |
| Internal rotation [Knee Flexed at 90°] | External rotation [Knee Flexed at 90°] |
| Semimembranosus Semitendinosus Gracilis Sartorius Popliteus |
Biceps femoris |
You would get a visual idea by watching the knee movements.