Last Updated on June 3, 2020
Congenital muscular torticollis is an asymmetrical deformity of the head and neck in which the head is tilted toward the side with the shortened muscle and the chin rotated towards the opposite side. The deformity is noticed after the birth of the child and it could manifest in a few days to weeks.
The deformity occurs due to the contracture of the sternocleidomastoid muscle on one side.
Congenital muscular torticollis is the most common cause of infantile torticollis.
The term torticollis is derived from two Latin words, tortus, meaning “twisted,” and collum, meaning “neck”.
Wryneck is a lay term is used to describe torticollis arising from any cause.
Congenital muscular torticollis is more common in girls than in boys.
The right side is involved in about 75 percent of cases of congenital muscular torticollis.

Etiology of Congenital Muscular Torticollis
The immediate cause of the deformity in congenital muscular torticollis is fibrosis within the sternocleidomastoid muscle, which subsequently contracts and shortens.
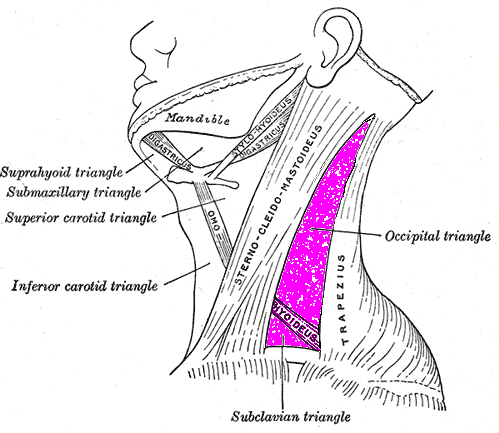
The sternocleidomastoid muscle arises from clavicle [clavicular head and sternum [sternal head] and attaches at the mastoid process behind the ear.
The contracture of sternocleidomastoid leads to a rotational deformity in the neck [The neck rotates to turn away from the affected side and tilts toward the affected side.]
The contracture occurs probably as a result of intrauterine compartment syndrome of the muscle thought. This compartment syndrome is believed to be caused by a venous outflow obstruction.
Many conditions can be associated with congenital muscular torticollis. These are
- Development dysplasia of hip
- Metatarsus adductus
- Trauma during delivery
- Asymmetric flattening of the skull [plagiocephaly]
- Congenital atlanto-occipital abnormalities
Except for trauma, interestingly, all other associated conditions have a common factor of reduced intrauterine space as one of their etiology.
The contracture in congenital muscular torticollis needs to be treated otherwise secondary deformities may develop as follows
- The face on the side becomes flattened because of external pressure as
- the infant usually sleeps in a prone posture
- the neck is rotated so that the affected side is down
- This results in ipsilateral the face is flattened by remodeling to conform to the bed.
With skeletal growth following changes occur
- Asymmetry of the face increase
- Levels of the eyes and ears change
- to accommodate tilt
- more pronounced when the head and neck are brought straight in the midline.
- cause ocular imbalance
- Cervical scoliosis with concavity towards the affected side
- Further soft-tissue contractures of the affected side – deep cervical fascia, the scalenus anterior and medius muscles become shortened and carotid sheath.
In very rare cases, both sternocleidomastoid muscles are affected. The condition is called double torticollis and is characterized by short neck, elevated chin, and upward tilted face.
Clinical Presentation
The deformity may be present at birth or it may become evident about the second or third weeks. The parents usually note the tilt and rotation of the head. The deformity becomes more evident when the child is able to support his neck as a developmental milestone.
On examination,
-the head is tilted towards the side of the affected muscle
– chin is rotated to the opposite side.
– Limitation of the movements
- Rotation of the neck to the side of the deformity
- Tilting the neck as to touch opposite shoulder with ear
On palpation, a hard, nontender, fusiform swelling, or tumor as it is also called, in the sternocleidomastoid muscle may be revealed. It becomes more prominent by a head tilt towards the affected side and chin rotation to the opposite side.
The band is typically not painful.
In delayed presentations, facial and head abnormalities may be seen.
Differential Diagnosis
- Postural torticollis
- Cervical hemivertebra
- Unilateral atlanto-occipital fusion
- Klippel-Feil syndrome
- Unilateral congenital absence of sternocleidomastoid muscle
- Pterygium colli
- C1, C2 rotatory subluxation
- Eye disorders
- Vestibular disorders
Imaging
The diagnosis is mainly clinical and images are not required for this purpose. However, it is important to rule out congenital abnormalities of the neck and this is where imaging has its role.
X-rays are especially indicated if no palpable mass present. This is to rule out other conditions that cause torticollis like rotatory atlanto-axial instability Klippel-Feil syndrome.
Ultrasound can help differentiate congenital muscular torticollis from other underlying neurologic or bony abnormalities.
CT Scan is done to rule out atlantoaxial rotatory subluxation.
Treatment of Congenital Muscular Torticollis
Nonoperative Treatment
Treatment of congenital muscular torticollis should be begun as soon as the diagnosis is made. Nonoperative treatment includes manipulations by parents as instructed. The manipulations consist of passive stretching of contracted sternocleidomastoid and other measures.
Passive Stretching
Passive stretching is indicated only if the condition is present for less than one year. Early intervention yields better results. About ninety percent of cases respond well to manipulation including the plagiocephaly remodeling.
For stretching, the head is bent laterally so that the ear on the side opposite the shortened muscle approaches the shoulder, then the head is rotated so that the chin approaches the shoulder on the affected side.
All the while, the neck should be in a comfortable hyperextended position. Countertraction should be applied by holding the ipsilateral shoulder and chest.
Another method of stretching the sternocleidomastoid muscle is by placing the infant supine on the mother’s lap with the head hanging into hyperextension. One hand stabilizes the shoulders and chest, and the other hand tilts the head laterally away from the contracted muscle so that the contralateral ear touches the opposite shoulder. The chin is then rotated toward the contracted muscle.
The muscle is stretched in one go for about 10 seconds and should be stretched 4 to 6 times a day.
Posture
It helps to keep the crib turned so that the infant’s unaffected side is against the wall and he will rotate his head to look toward the involved side when his attention is attracted, actively stretching the muscle when reaching and grasping for toys.
Prone posture during sleep should be avoided.
Operative Treatment
If the stretching exercises are begun at a very early age and performed faithfully and correctly every day, the deformity and contracture correct and surgery is often not required.
Surgery is indicated in cases that do not respond to stretching up to one year of age. Fibrous cord and late presentation are often causes of poor response.
Surgery involves cutting of both the ends of the muscle so that it can be lengthened by stretching as it heals. This surgery is called a bipolar release.
When only one end is cut, it is called unipolar release. In severe cases, the release may be required in both upper and lower end of the muscle.
The muscle may be divided at either end or at both ends.
Postoperative immobilization in overcorrected position is maintained for about 6-8 weeks.
Complications of Congenital Muscular Torticollis
If patient is left untreated, the following complications may be seen