Last Updated on December 22, 2019
Fractures in children demand special consideration because the skeleton of children though resembles adult skeleton is kind of different. Anatomically as well as physiologically, bones in children are quite different from adult bones.
Roughly about one-third of children have had a fracture by the age of 18. Fractures of the forearm are the most common injuries of the children.
Children are quite active physically and often adventurous, making them more vulnerable to trauma.

How Does Child Bones Differ From Adult?
Bones in children have great healing power and fractures in children almost always unite. It is rare to find a fracture not uniting in case of fractures in children and whenever it occurs, there would be a strong reason for it like infection or some other pathology.
Bones of children are softer and pliant as compared to adult bones. To compare imagine a twig and a hard stick. Because of this bones in children can absorb a greater trauma without getting fractured.
Periosteum, the layer that covers the bones, in children is quite thick in comparison to the adult periosteum. It is difficult to tear easily because of thickness and thus prevents the displacement of fractured pieces.
The rate of healing of fractures in children is faster than that in adults. This rate decreases with the age of the child.
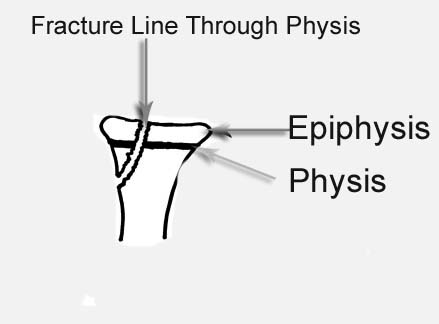
One another big difference in bones of children are is the growth of the bone. This growth occurs at the bone ends which harbor a growth plate called physis. Physis is separated from the joint by a bony tissue called epiphysis. Injury to this physis or growth plate is a peculiar phenomenon in children because the growth plate ceases to function and fuses with the bone after completion of growth.
Fractures in children can occur due to accidents, child abuse or due to some pathologies. Motor vehicle accidents and falls from a height account for major mechanisms of accidental trauma causing fractures in children.
Some fractures are known to occur more in specific age groups. For example, fractures of the femur are most common in children ages 0 to 3 years of age. Similarly, fractures of the supracondylar area in humerus are more common in the second decade and the peak is around 7 years of age.
Physeal fractures are more common near skeletal maturity.
Distal Forearm, phalanges, proximal humerus peak around 14 years of age. Clavicle, Femur, foot bones, forearm bones have peak incidence of fractures around 5 years and 15 years whereas ankle, carpal metacarpal rise linear with age. Diaphyseal fractures showed an irregular pattern.
In children, the upper is injured much more commonly than the lower limb. The distal radius is the most common fracture in the upper limb followed by the elbow.
Physeal injuries constitute 14.5% – 27.6% of pediatric injuries. Open fractures constitute about 3% of the injuries are open fractures
Multiple fractures in children are uncommon.
Epidemiology of Fractures in Children
It is estimated that each year 1.6% to 2.1% of all the children sustain a fracture. Fractures in children show a linear increase with age, peaking at 12 years and then decrease until the age of 16 years.
Overall accidental injury is most commonly responsible for the fractures in children. However, in first year, child abuse is most common cause in Western world [Clear data for the rest of the world not available]
Boys are affected almost 3 times more than girls but the ratio vary from region to region.
Fractures are more common during the summer [Except in infants] due to more hours avaiable for activity.
Types of Fractures in Children
There are few fractures that occur in children only. These fractures are
Greenstick fractures
As bones of children more pliable than adult bone, a fracture pattern may occur in which fracture is not complete. Such fracture are called Greenstick fractures. In this one side of the bone breaks and one side is bent.
The name for a greenstick fracture comes from the analogy of breaking a young, fresh tree branch. when you try breaking a fresh tree branch it snaps on the outer side of the bend while the inner side is bent, and still in continuity.


Though incomplete, the greenstick fracture must be bent back into the proper position and then plaster should be applied for an appropriate time so as to maintain the position till the fracture unites.
Torus Fractures or Buckle Fractures
Torus fractures in children are the fractures where one cortex of the bone bends (buckles) upon itself without breaking the other side. These are also called buckle fracture.

Epiphyseal Fractures
Injuries to the growth plate or physis are restricted to child skeleton. This is because after puberty the physis fuses with the bone. These injuries are called epiphyseal injuries and can result in stoppage of growth and bone shortening.
Causes of Fractures in Children
Accidental injuries are the most common cause of fractures in children. Accidental trauma can occur in a variety of settings and can be considered to occur in the following five environments-
- Home
- School
- Play and recreational activities
- Motor vehicle and road accidents
- Uncommon causes are ice cream truck, water tubing, gunshot wounds etc.
A child with multiple fractures not fitting into an injury pattern should be suspected to have child abuse.
Clinical Presentation of Fractures in Children
Very young children after injury will cry and would restrict the use of the injured area. Following are the most common symptoms of a fracture.
- Pain in the injured area
- Swelling in the injured area
- Warmth, bruising, or redness in the injured area
- Deformity
- Difficulty using or moving the injured area in
In severe injuries,a fter the initial resuscitation and stabilization, the child is assessed from head to toe and injuries in the head, face, cervical spine, chest, abdomen, pelvis, spine, and extremities.
The severity of the injuries can be scored by using a scoring system like Injury Severity Score or Pediatric Trauma Score.
The scoring system assesses mortality risk at the time of initial treatment, as well as allowing some degree of prediction of future disability.
For head injury, Pediatric Glasgow Coma Scale is used.
If an extremity is injured, note should be made if the injury is closed or open. Any active bleeding should be stopped by a pressure bandage.
Imaging
As with adults, xray is the first investigation and would suffice in most of the cases.
In a fracture with preexisting pathology, other investigations like CT or MRI may be required.
Radiographs
After the initial resuscitation and physical examination, X-rays are done. Any limb with a significant injury should be examined on x-ray. In the presence of head injury or suspected neck injury, a lateral cervical spine x-ray is obtained.
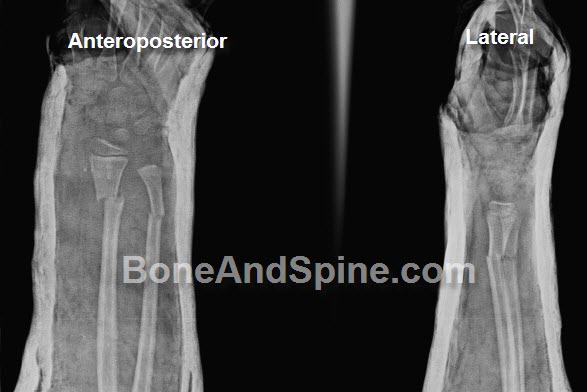
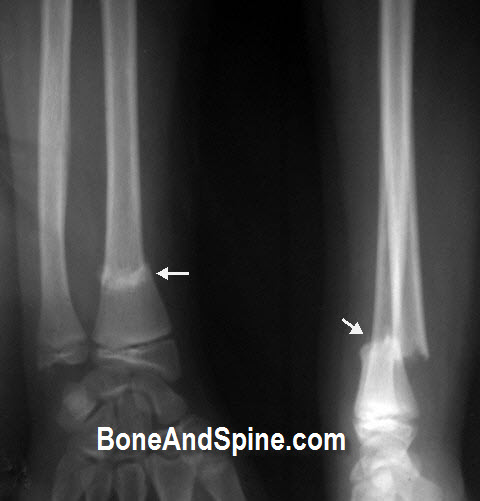
Following are x-rays of forearm fractures in children


Computed Tomography
Computed tomography is essential in a child with multiple injuries.
Ultrasound
Ultrasound is very helpful in abdominal injuries. It is very accurate means for detecting hemoperitoneum following injury. But ultrasound reporting is dependent on the operator and in comparison, CT is superior for diagnosing visceral injury in children.
Magnetic Resonance Imaging
The primary use of magnetic resonance imaging is for the detection of injury to the brain or the spine and the spinal cord. In SCIWORA syndrome, MRI demonstrates the site and extent of spinal cord injury and in defining the level of injury to the disks or vertebral apophysis.
MRI also is very useful in evaluating knee injuries that cannot be visualized on routine x-rays.
Treatment of Fractures in Children
The first priority in an injured child management of the life-threatening, injuries if present.
As in trauma management, care of airway, breathing, and circulation takes precedence followed by cervical spine stabilization.
Fluid replacement is done to compensate for the loss from hemorrhage, initially with an intravenous crystalloid solution.
In very young children where rapid intravenous access may be difficult, intraosseous fluid infusion through tibia may be considered using an intraosseous route.
Death is common if the hypovolemic shock is not rapidly reversed but the excessive fluid replacement also may lead to interstitial pulmonary edema. A urinary catheter is essential during the resuscitation to monitor urine output and to gauge adequate organ perfusion.
Most of the fractures in children are treated by nonoperative means which include splints, plaster casts, and traction.
Surgery is being done for many a fracture like epiphyseal fractures, intraarticular fractures, and long bone fractures after a certain age to limit the time on the bed and increase early mobility.
Pathological Fractures in Children
A pathological fracture is defined as a fracture that occurs through abnormal bone, a bone that lacks normal biomechanical and viscoelastic properties.
Pathological fractures may result from generalized bone weakness caused by an external process like radiation. Another example of the external cause is a hole caused by a procedure like fixation or biopsy.
Most of the fractures, however, have internal causes that could be localized or generalized.

Generalized bone Diseases Causing Pathological Fractures In Children
- Rickets
- Osteogenesis imperfecta
- Osteopetrosis
- Antley-Bixler syndrome
- Cytochrome P450 oxidoreductase deficiency
- Jaffe-Campanacci syndrome
- Bruck syndrome
- Malabsorption syndrome
- Cushing’s syndrome
- Scurvy
- Carbonic anhydrase type 2 deficiency
- Metastases
- Hypophosphatasia
- Polyostotic osteolytic expansile dysplasia
- Copper deficiency
- Osteoporosis-pseudoglioma syndrome
- Pyknodysostosis
- Hyperparathyroidism
- Osteoporosis
- Anorexia nervosa
- Gorham’s vanishing bone disease
Localized Conditions Causing Pathological Fractures In Children
- Enchondroma
- Infection-Osteomyelitis
- Bone Tumors – Benign and malignant
- Tumor like lesions of bone
- Bone Cyst
- Retrauma in recently united bone
Pathological fractures are special as apart from the fracture, pathology also needs to be managed.
Treatment of Fractures in Children
Children have great potential for healing. The immature skeleton heals faster. Therefore a fracture in a younger child would heal in lesser time than that of an older child. The healing capacity or potential is maximum in the newborn and decreases as the child grows to reach an adult value.
Treatment of an individual fracture depends on the type of fracture and the associated injuries. The general approach is as follows
Treatment will also depend on symptoms of the child [severity], age, and general health. It will also depend on how severe the condition is.
For example, an open fracture is an emergency and needs urgent attention, and often surgery. Most of the closed fractures can be treated.
Following are the methods to treat fractures in children-
Splint or cast
Most of the fractures in children respond very well to casting or splining. Displaced fractures are reduced and held in place with the use of plaster cast.
Traction
Traction is used as a treatment of fractures in children a lot more than adults. But because it requires aggressive in-hospital monitoring till bone sufficiently unites, and there are better surgical alternatives available now, the popularity is decreasing.
In small children fracture of femur is famously treated with traction.
Surgery
As of today, more surgical procedures are being performed on children than in the past. This comes from the availability of better implants, ideal parental expectations, better and easier self/supervised care after surgery.
Some of the fractures in children are a surgical emergency and need urgent surgical intervention. For example fracture neck of femur.
Complications
Nonunion is a relatively rarer problem as compared to adult fractures. This is because of the higher potential of children’s bones to unite.

Malunion can occur due to unacceptable reductions or neglect.

Refracture can occur due to reinjury or indulging in activities before the fracture has consolidated enough.
Growth disturbancs can occur in epiphyseal fractures where physeal injury is severe or reductions are not anatomical.