Last Updated on November 1, 2019
Base of thumb fractures are the extra-articular and intraarticular fractures of base of first metacarpal bone.
Thumb is a highly important and efficient digit that makes the human hand highly efficient. An unusable thumb could mean a loss of 40% of hand function.
Relevant Anatomy
[Read complete hand anatomy]
Thumb consists of two phalanges and a metacarpal. The metacarpal consists of a base, shaft and head like other metacarpals. which articulates.
The base of thumb has an articular region that articulates with the trapezium bone.
The metacarpophalangeal joint has 6 degrees of freedom and produces motion of flexion and extension, abduction and adduction, and pronation and supination.

The following structures stabilize the joint
- Volar oblique ligaments
- Volar oblique originates on the trapezium and inserts into the volar beak of the thumb metacarpal.
- The most important ligament in maintaining stability
- Volar and dorsal oblique ligaments
- Dorsal oblique
- Not as strong as volar oblique ligament
- Reinforced by abductor pollicis longus
- Anterior and posterior intermetacarpal ligaments
- Dorsal radial ligament
- The proper collateral ligament
- Arises from the lateral condyles of the metacarpal
- Inserts on the volar aspect of the proximal phalanx
-
- Tight in flexion and loose in extension
- Accessory collateral ligament
- Arises from the metacarpal neck
- Inserts into the volar plate and the sesamoids
- More volar in location than the proper collateral ligament
- Tight in extension and loose in flexion
Muscles attaching on to thumb
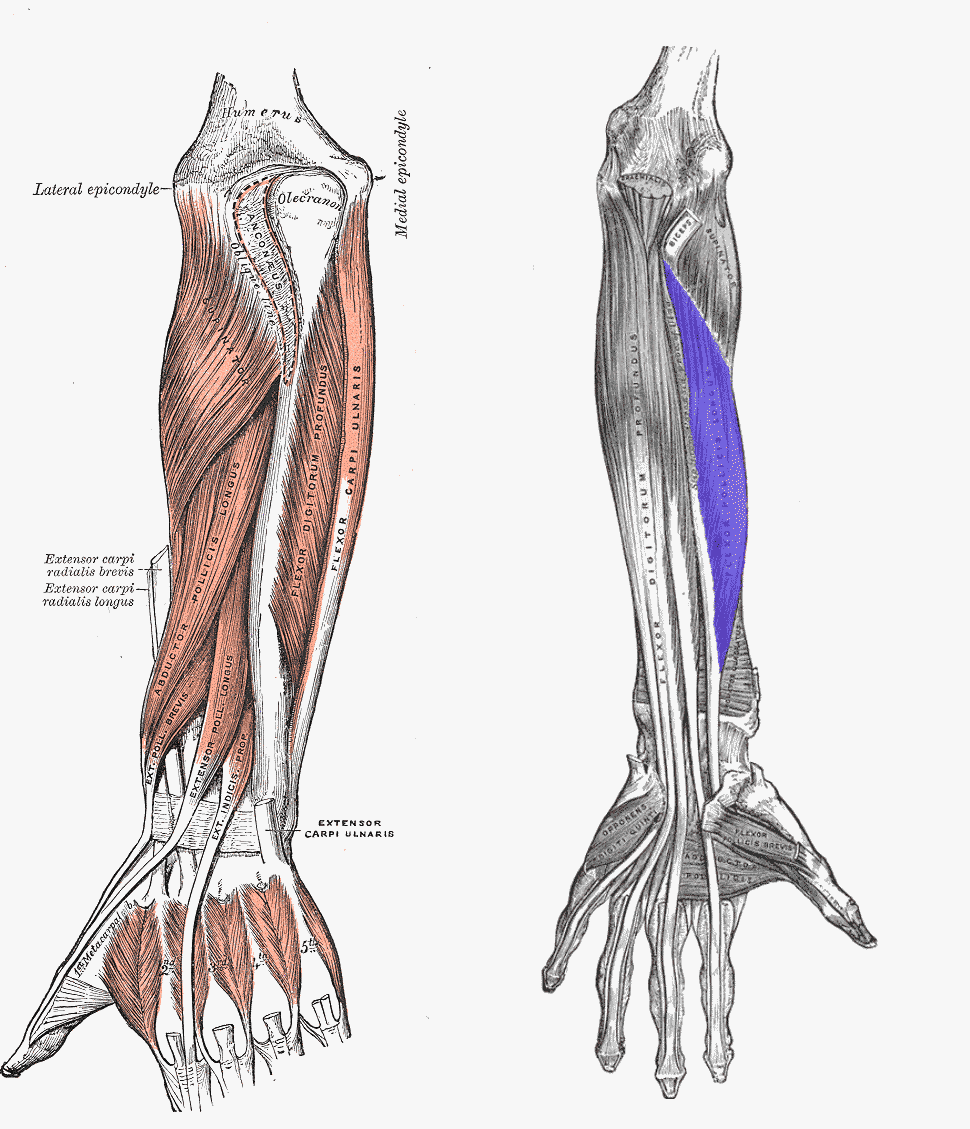
Extrinsic Muscles
- Flexor pollicis longus
- It originates on the anteriorly distal to the radial tuberosity and interosseous membrane.
- Attaches onto the base of the distal phalanx of the thumb.
- Flexes thumb
- Supplied by anterior interosseous [median nerve branch] nerve
- Abductor pollicis longus
- Originates from dorsal sides of both the ulna and the radius, and interosseous membrane
- Inserts to the base of the first metacarpal bone
- Abductor of thumb
- Supplied by radial nerve
- Extensor pollicis longus
- From the dorsal side of the ulna and the interosseous membrane
- Inserted onto the base of the distal phalanx of the thumb.
- Extensor of thumb
- Supplied by radial nerve
- Extensor pollicis brevis
- Originates on the dorsal aspect of ulna, interosseous membrane, and radius
- Origin is distal to the abductor pollicis longus origin
- Inserts on the base of the proximal phalanx of the thumb
- Extends and abducts the thumb
- Supplied by the radial nerve
Thenar Muscles

- Abductor pollicis brevis
- Originates from the scaphoid tubercle and the flexor retinaculum
- Inserts on radial aspect of the proximal phalanx and radial side sesamoid
- Supplied by the radial nerve
- Flexor pollicis brevis
- Two heads
- Superficial head arises on the flexor retinaculum
- Deep head originates on trapezium, trapezoid, and capitate.
- Inserted onto the radial sesamoid bone of the metacarpophalangeal joint
- Flexor, adductor and abductor of the thumb
- Therefore also able to oppose the thumb
- Dual nerve supply
- Superficial head-median nerve
- Deep head – ulnar nerve
- Two heads
- Opponens pollicis
- Originates from the tubercle of the trapezium and the flexor retinaculum
- Inserted on to the radial side of the first metacarpal
- Opposes the thumb and assists in adduction
- Supplied by the median nerve
- Adductor pollicis
- Two heads
- Transverse head – from the entire third metacarpal bone
- Oblique head- From the carpal bones proximal to the third metacarpal
- Inserts onto the ulnar sesamoid bone of the metacarpophalangeal joint
- Adducts the thumb, and assists in opposition and flexion
- Supplied by the deep branch of the ulnar nerve
- Two heads
Thus there are three muscles attaching to the base of the thumb. These muscles act as deforming forces when the fracture occurs at the base of the thumb. These are
- Abductor pollicis longus
- Extensor pollicis longus
- Adductor pollicis
There is a very limited rotation at the carpometacarpal joint.
There is an average of 53 degrees flexion-extension and abduction-adduction of 42 degrees
Types of Base of Thumb Fractures
Extraarticular fractures
These fractures are more common than intraarticular base of thumb fractures.
These occur at the proximal metaphyseal-diaphyseal junction. They could be transverse or oblique.
The distal fragment is adducted and flexed due to pull of adductor pollicis, abductor pollicis Brevis, flexor pollicis Brevis.
Intraarticular Fractures
The base of thumb fractures are further divided into Bennet, Rolando and Comminuted fractures
Bennett fracture
Benett fractures are the intra-articular base of thumb fracture where a single volar ulnar base portion remains intact held by a volar oblique ligament.
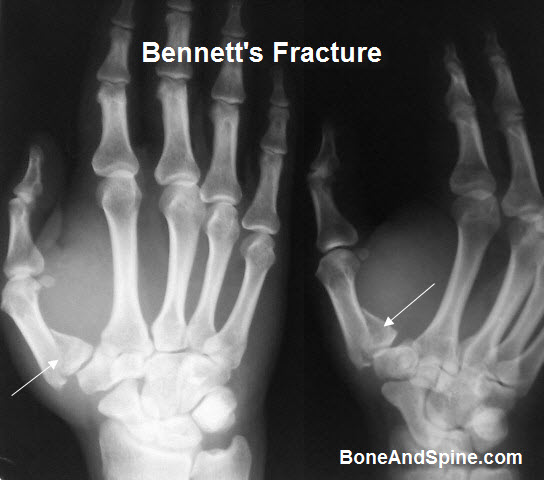
The displaced metacarpal is pulled dorsally and radially by the abductor pollicis longus, adductor pollicis and thumb extensors
Rolando fracture
It is a 3 part intraarticular base of thumb fracture. It is usually seen as T or Y pattern fracture with both volar and dorsal fragments is present.

Volar carpal ligament remains attached to the volar fragment. Adductor pollicis longus remains with the dorsal fragment.
Rolando fracture is the least common type of the base of thumb fractures.
Comminuted fractures
These fractures are common and produce varying degrees of articular surface impaction.
Mechanism of injury
Both direct and indirect trauma can result in base of thumb fractures. intraarticular fractures occur when the axial force is applied to the thumb in the flexion.
Clinical Presentation
Pain, swelling is present on radial side, in the region of the snuffbox.
The thumb may appear shortened or deformed and is painful to move at the carpometacarpal joint.
Tenderness is present in the region of the injury.
Imaging
X-rays of the thumb are taken with a focus on the digit are taken. In most cases AP and lateral views are sufficient. But special views may be needed.
- True AP of thumb (Robert’s View)
- Arm in full pronation with dorsum of thumb on cassette
- True lateral of thumb
- hand pronated 30 degrees and beam angled 15 degrees distally
- Traction view
- For better understanding of fracture pattern
- Especially done in Rolando and severely comminuted base of thumb fractures
Bennet’s fracture is characterized by a small fragment of 1st metacarpal base articulating with trapezium.
Rolando fracture shows a typically Y shaped intraarticular fracture due to splitting of the metacarpal base into volar and dorsal fragments
Treatment
Extra-articular fractures are treated generally by closed reduction and thumb spica cast.
Transverse fractures generally are stable whereas oblique fractures may displace and require surgery.
Other indications for considering surgical treatment are
- Angulation greater than 30 degrees
- Comminuted fractures with shortening
- Open fractures
In surgery, closed reduction and percutaneous K-wire fixation is the procedure of choice. Open reduction is rarely required.
Bennett fracture
- With less than 1 mm displacement is also treated with closed reduction and thumb spica cast immobilization.
- Greater than 1 mm of articular incongruity after closed reduction indicates operative intervention
- In cases where reduction is not stable closed reduction and pinning [k-wiring] is preferred.
- Open reduction with k-wire fixation may be required in certain cases
Rolando fracture
- The articular incongruity and fragment size determines the treatment pattern
- Nondisplaced fracture with articular incongruity less than 1 mm – percutaneous pin fixation
- More than 1 mm of incongruity
- Open reduction or
- Distraction and external fixation
Comminuted fractures
- Ligamentotaxis or distraction and external fixation
Surgical Procedures
Closed reduction and percutaneous k-wire fixation
- Transverse extra-articular fracture
- A transarticular wire can be used
- Oblique extra-articular fractures
- Intermetacarpal k-wire fixation
-
- loss of reduction can occur and should be watched for
Open reduction internal fixation
-
-
- volar approach
- Fracture provisionally reduced with k-wire and fixed with screws or T-plate depending on fracture pattern
-
Distraction and external fixation
- Two 3mm K-wires in the dorsoradial aspect of the distal shaft of the metacarpal
- Similar wires are placed in the dorsoradial aspect of the radius
- These two sets of k-wires are connected with a bar and fracture is reduced with distraction
- Pin site infection is a known complication
Complications
- Posttraumatic arthritis
- Risk factors
- Highly comminuted intra-articular fracture
- Major step off
- Multiple small fragments
- Risk factors
- Malunion
- Stiffness
- Degenerative arthritis in nonanatomical reduction of intra-articular fractures
- Loss of motion
- Prolonged immobilization
- Adhesions
Prognosis
The severity of the initial injury determines the prognosis.
Anatomical restoration is associated with better function and decreased risk of complications.
Imperfect reductions and above forces lead to increased joint contact pressures and subsequent predisposition to early arthritis.
References
- Abid H, Shimi M, El Ibrahimi A, El Mrini A. Articular fracture of the base of the thumb metacarpal: comparative study between direct open fixation and extrafocal pinning. Chir Main. 2015 Jun. 34 (3):122-5.
- Soyer AD. Fractures of the base of the first metacarpal: current treatment options. J Am Acad Orthop Surg. 1999 Nov-Dec. 7(6):403-12.