Last Updated on January 29, 2024
Distal radius fracture refers to fractures that can be either extra-articular or intraarticular fractures of distal end of the radius. The treatment of these fractures varies with the type of fracture, the age of the patient, associated soft tissue injury and demand of the patients. While fractures in younger patients demand an aggressive approach, older patients with lesser demand have a high acceptability of conservative treatment.
Distal radius fractures have peaks of occurrence in children ages 5 to 14 years and adults >50 years. In elderly patients, it is an insufficiency fracture while in younger males it is a traumatic injury.
Many of the fractures of distal radius are known by their eponyms. The Colles’ fracture, the Smith’s fracture, and the Barton’s fractures are few of the common names.
Distal radius fractures are the most common osteoporotic fractures and represent up to 25% of the fractures seen clinically. These fractures are seen more commonly in females.
Relevant Anatomy of Distal Radius
[read more about anatomy of radius bone]
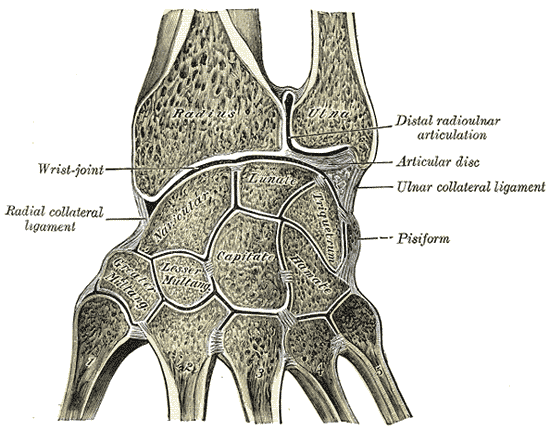
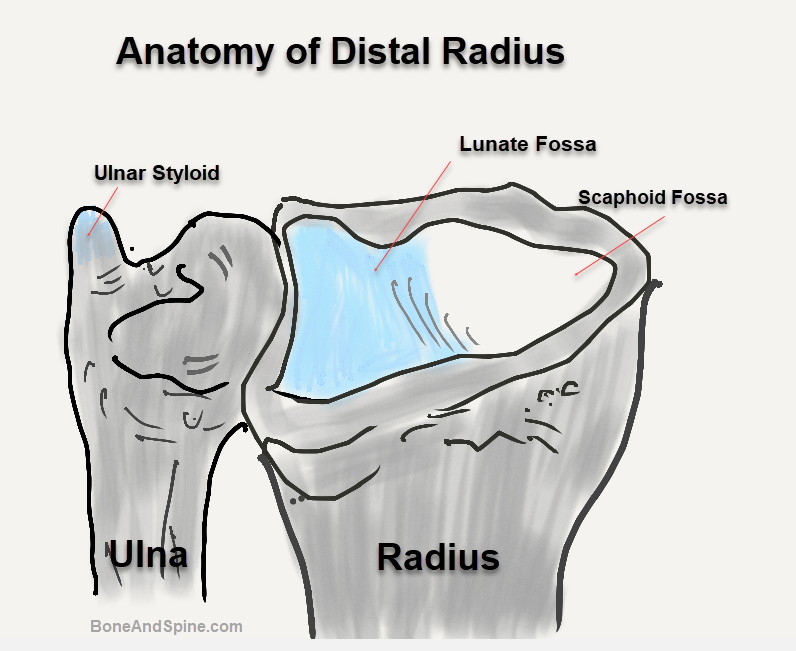
Distally, the radial shaft expands to form a rectangular end. The lateral side projects distally as the styloid process. In the medial surface, there is a concavity, called the ulnar notch, which articulates with the head of the ulna, forming the distal radioulnar joint.
The distal surface of the radius has two facets, for articulation with the scaphoid and lunate carpal bones. This makes up the wrist joint.
The distal radius is made up of the metaphysis and three articular surfaces and is responsible for 80% of the axial load. It articulates with
- Laterally the scaphoid facet
- Medially, the lunate facet
- Sigmoid notch for distal radioulnar joint
Distally, the radius has a somewhat trapezoidal shape. The radial styloid rotates palmarly 15 degrees off the axis of the radius. The articular surface has an inclination of 21 degrees in the anteroposterior plane and 5 -11 degrees in the lateral.
The radius has a thin cortical bone on the dorsal and radial aspect making the fractures typically collapse dorsoradially. The palmar ulnar cortex is strong and dense relatively. The palmar ulnar part is often referred to as the keystone of the radius. It serves as the attachment for the palmar distal radioulnar ligaments and also the radiolunate ligament. Displacement of this fragment is associated with palmar displacement of the wrist bones and also with the loss of forearm rotation.
The triangular fibrocartilage extends from the rim of the sigmoid notch of the radius to the ulnar styloid process.

The ulna plays an important part in the ligamentous integrity of the distal radio-ulnar joint and triangular fibrocartilage.
Attachments to distal radius are
- The brachioradialis inserts on the lowest part of the lateral surface just above the styloid process.
- The pronator quadratus is inserted into the lower part of the anterior surface and into the triangular area on the medial side of the lower end.
- The articular capsule of the wrist joint is attached to the anterior and posterior margins of the inferior articular surface.
- The extensor retinaculum is attached to the lower part of the anterior border.
- The interosseous membrane is attached to the lower three-fourths of the interosseous border.
- The articular disc of the inferior radioulnar joint is attached to the lower border of the ulnar notch
Columns of Wrist
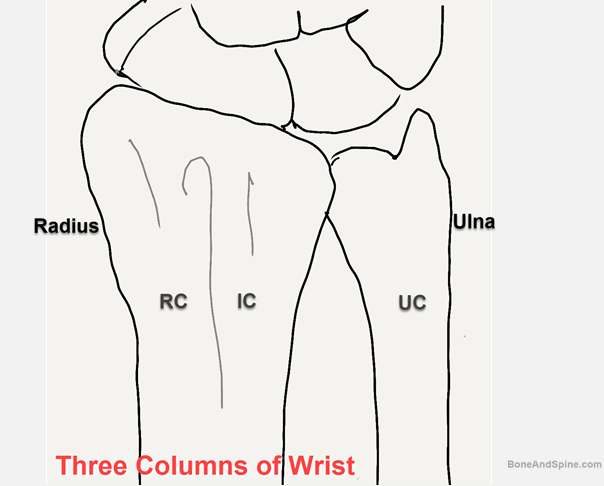
The wrist is said to consist of three distinct columns, each of which is subjected to different forces and must be addressed as discrete elements.
- Radial column: It includes the scaphoid fossa and the radial styloid. It is best stabilized by buttressing the lateral cortex. Provides attachment to the brachioradialis tendon, long radiolunate ligament, and radioscaphocapitate ligament. It resists radial carpal translation and acts as as a load-bearing site for activities performed in ulnar deviation. Radioscaphocapitate ligament that attaches to it prevents lnar translation of wrist bones.
- Intermediate column: It consists of the lunate fossa and the sigmoid notch of the radius. It is critical for both articular congruity and distal radioulnar function. It also transmits load from carpus to forearm.
- Ulnar column: consists of the ulnar styloid with TFCC and the ulnocarpal ligaments. It is involved in integrity of distal radioulnar joint and forearm rotatory motion.
The ulna plays an important part in the ligamentous integrity of the distal radio-ulnar joint and triangular fibrocartilage.
Biomechanics of Wrist
The palmar extrinsic ligaments are relied on to reduce the components of a fracture using closed methods.
The palmar ligaments are stronger than the thinner dorsal ligaments and more vertically oriented than dorsal ligaments. Any force applied would make palmar ligaments taut before the dorsal ligaments bringing the palmar cortex to length before the dorsal cortex.
Associate Injuries
Distal radius fracture in the elderly is caused by a fall on the outstretched hand or FOOSH. However, in young persons, it is a high-energy fracture and may be associated with the following injuries
- Radial styloid fractures
- Distal radioulnar joint injury
- TFCC injury
- Scapholunate ligament injury
- Lunotriquetral ligament injury
Classification of Distal Radius Fractures
Several distal radius fracture classification systems have been proposed for fractures of the distal radius. Here are the major ones used widely
Gartland and Werle
A distal radius fracture classification system that assessed the three basic components of these injuries
- Metaphyseal comminution
- Intra-articular extension
- Displacement of the fragments.
Fractures are classified into four groups
- Group I: Simple Colles’ fracture with no involvement of the radial articular surfaces
- Group II: Comminuted Colles’ fractures with the intraarticular extension without displacement
- Group III: Comminuted Colles’ fractures with intra-articular extension with displacement
- Group IV: Extra-articular, undisplaced
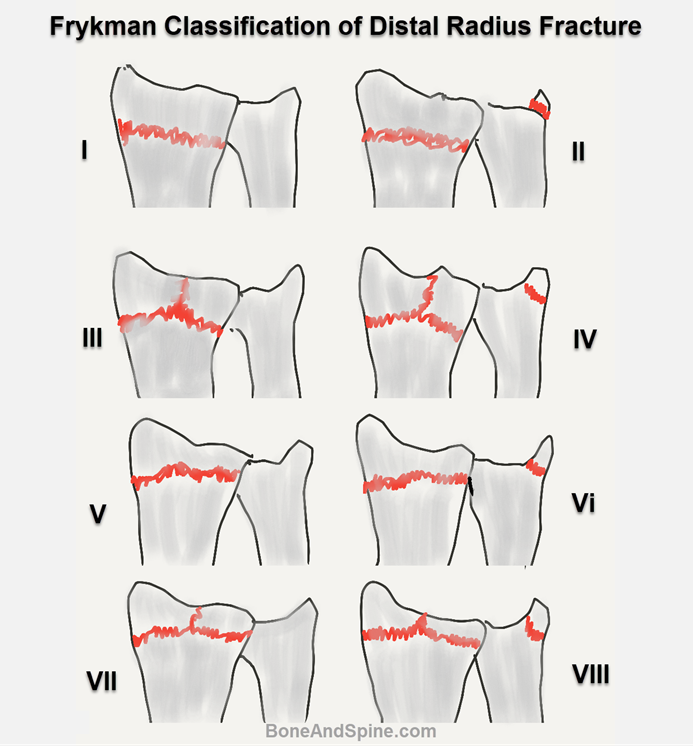
Frykman
It included individual involvement of the radiocarpal and radioulnar joints-
- Type I: Extra-articular fracture
- Type II: Extra-articular fracture with the ulnar styloid fracture
- Type III: Radiocarpal articular involvement
- Type IV: Radiocarpal involvement with ulnar styloid fracture
- Type V: Radioulnar joint involvement
- Type VI: Radioulnar joint involvement with ulnar styloid fracture
- Type VII: Radioulnar and radiocarpal joint involvement
- Type VIII: Radioulnar and radiocarpal joint involvement with ulnar styloid fracture
AO Distal Radius Fracture Classification
Fractures are classified with the increasing severity of the bony injury:
- Type A: Extra-articular fracture. Subgroups are based upon angulation and comminution
- Type B: Partial articular fracture. Subgroups are based upon lateral (radial styloid) palmar or dorsal fragments
- Type C: Complete articular. Subgroups are based on the articular surface’s degree of comminution and the metaphysis
Fernandez
Fernandez proposed a mechanism-based classification system. It is based on the mechanism of injury. It also addresses the potential for ligamentous injury and also guides the treatment but is little complex to use.
- Type I: Metaphyseal bending fractures with loss of palmar tilt and radial shortening relative to the ulna (Colle’s and Smith fractures).
- Type II: Shearing fractures of joint surfaces requiring reduction and often buttressing of the articular segment. (Barton fracture and fracture of radial styloid)
- Type III: Compression of the articular surface without the characteristic fragmentation; also includes the potential for significant interosseous ligament injury. (Die-punch fracture)
- Type IV: Avulsion fractures or radiocarpal fracture-dislocations. (Fractures of radial and ulnar styloid)
- Type V: Combined injuries with significant soft tissue involvement due to the high-energy nature of these fractures.
There is also a separate grouping of the possible associated distal radioulnar joint lesions.
Melone
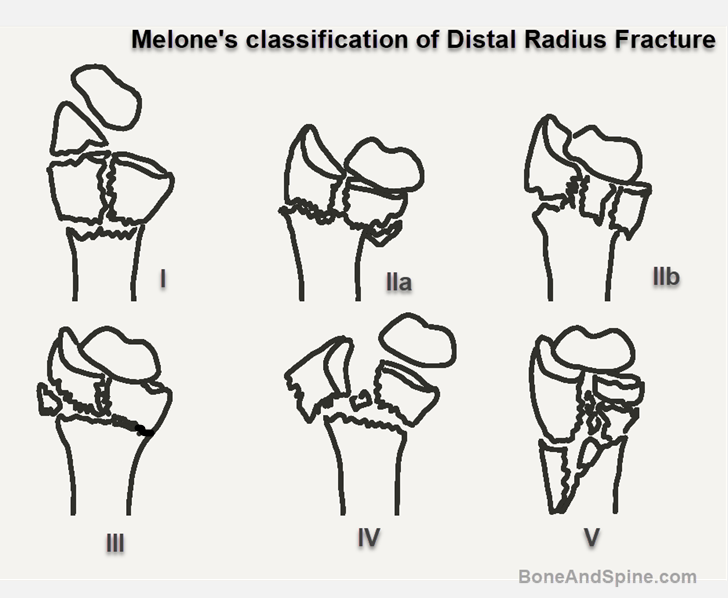
Melone outlined a classification of intraarticular fractures of the distal radius. It is based on the observation that there are four components to radiocarpal intraarticular injuries- radial shaft, radial styloid, dorsal medial fragment of lunate facet, and palmar medial fragment of lunate face
- Type I: Undisplaced or medially displaced components. Can be managed without surgery
- Type II: Significant displacement of the medial component as a unit with comminution of metaphyses (IIa- reducible, IIb- irreducible) [Die punch fracture with moderate to severe displacement]
- Type III: Type II fracture with a spike of radial shaft spike fragment present
- Type IV: Severe disruption of the radial articular surface and dorsal and medial fragment wide apart. Extensive soft tissue damage. (split fracture)
- Type V: Crush and compression severe injury with extensive comminution
Universal Classification
The Universal classification is an attempt to improve on the Frykman classification. It makes a distinction between displaced and nondisplaced, and extra and intra-articular fractures. It is quite simple and straightforward
- I- Extraarticular undisplaced
- II- Extraarticular displaced
- III -Intraarticular, undisplaced
- IV- Intraarticular, displaced
- IVa – reducible
- IVb- reducible but unstable
- IVc- Unreducible
Communication Terms Used in Describing Distal Radius Fracture
In spite of different comprehensive systems available, there is no universal classification system and different eponyms and terms are regularly used to convey the fracture pattern. This usage is across various systems of classification and is used for the cultural continuance and convenience of conveying.
Various eponyms used in distal radius fractures are
- Colles’ fracture: Often seen in the elderly. It is a low-energy extraarticular fracture with dorsal displacement.
- Smith’s fracture: It is similar in all aspects to Colle’s but the displacement is volar.
- Barton’s fractures: Intra-articular fracture of radius involving the volar or dorsal lip (called volar Barton or dorsal Barton). It is a kind of fracture-dislocation of the radiocarpal joint.
- Chauffer’s fracture: Fracture of radial styloid
- Die-punch fracture: Depressed fracture of the lunate fossa of the articular surface of the radius
How to describe a distal radius fracture
To describe a fracture, see whether
- Extraarticular or involves the joint
- Displacement of extraarticular fracture or displacement of major intraarticular fracture
- Involves the ulnar styloid or not
- Comminuted
Thus labeling it as – a left radius extraarticular distal end fracture with dorsal displacement conveys the same meaning as Colle’s fracture.
Presentation Fractures of Distal Radius Fracture
There is often a history of falls on the hands of the involved side. The patient presents with wrist pain, deformity, and swelling of the wrist.
On physical examination, ecchymosis and swelling is usually noticed. There would be visible deformity in case of displaced fractures and the part would be tender.
Other parts of the limb that are required to be seen in the examination are the ipsilateral shoulder and elbow.
The fracture may often be associated with fractures of either the same limb’s radial head or supracondylar humerus. When associated with these fractures, it indicates a high-energy trauma and may pose rehabilitation challenges
Ipsilateral radial head and distal radial fractures may indicate that sufficient energy has been imparted to result in injury to interosseous membrane (structure spanning between radius and ulna) an Essex-Lopresti lesion.
A thorough evaluation of the hand muscles and nerve function should be done.
Median nerve injury is a common cause of functional impairment and chronic pain. Because of dorsal angulation, the palmar portion [on the side of the palm] of the fragment becomes prominent, it might result in the displacement of the median nerve palmar ward.
This displacement of the nerve and the associated hematoma in the carpal tunnel may result in symptoms of acute carpal tunnel syndrome.
The acute shortening of the radius relative to the ulna may also cause the ulna to cause a wound on the palmar side.
Imaging
X-rays
The initial investigation is an x-ray of the wrist. The views include anteroposterior, lateral, and pronator oblique views.
PA View

If a fracture is extra-articular [ Does not involve the joint] radial shortening and comminution are noted. In addition, if present, the location of fracture of the ulnar styloid is noted (tip/waist/base).
In the case of intra-articular fractures, any impacted fragment including depression of the lunate facet is noted [articular surface of distal end radius for lunate bone] is looked for. Interruption of the proximal carpal row, if any would be visible on this view.
Lateral View

Palmar tilt, the extent of metaphyseal comminution, displacement of the volar cortex, the scapholunate angle, and position of the distal radioulnar joint are to be noted in extra-articular fractures.
Palmar Tilt represents the angle between a line joining the dorsal and volar margins of the articular surface and the long axis of the radius on a lateral x-ray.
For intra-articular fractures depression of the palmar lunate facet and/or depression of the central fragment, and the gap between palmar and dorsal fragments is noted.
Sometimes, tilted lateral views are done for a better view of the lunate facet as it eliminates the shadow of radial styloid
Oblique View
Oblique views are done for better assessment of radial comminution in extraarticular fractures or to look for radial styloid split/depression and depression of the dorsal lunate facet.
AP and lateral views of opposite sides are used to assess the patient’s normal values.
Distal End Radius X-ray Measurement Values – Normal and Abnormal

- Radial Inclination: The radial inclination is also termed the radial angle and is measure of slope of distal radial articular surface relative to the shaft. This measurement is taken in the posteroanterior radiograph of the wrist. Radial inclination represents the angle between one line connecting the radial styloid tip and the ulnar aspect of the distal radius and a second line perpendicular to the longitudinal axis of the radius.The radial inclination ranges between 21° and 25°. The radial inclination value would change in fractures of the articular surface. Loss of radial inclination will increase the load across the lunate.
- Radial Height: It is also called radial length and is measured on the posteroanterior radiograph. It is measured as the distance between the line perpendicular to the long axis of the radius passing through the distal tip of the radial styloid and along the articular surface of the radius. The average value of this measurement averages 8-13 mm. Loss of this height may occur in distal radius fractures and is called radial shortening.
- Volar tilt: The volar tilt, or volar inclination, or palmar tilt [Also called dorsal tilt] is measured on the lateral view. It is the angle between a line perpendicular to the long axis of the radius and a tangent line is drawn along the slope of the dorsal-to-volar surface of the radius.The normal angle is 7-15º. MOre than 10 degrees of dorsal tilt is related to worse outcomes.The term dorsal tilt is sometimes used if the angulation is dorsal rather than volar, negative values of volar tilt can be used instead to indicate a dorsal angulation. (Source- Radiopedia )
CT
CT is a better investigation to look for intra-articular extension and is more accurate. CT is also superior in defining step-offs (incongruency in articular surface) and gaps if any. CT is useful in the evaluation of complex or occult fractures, articular surface, and distal radio-ulnar joints. It may be indicated in occult fractures suspected on clinical examination but absent on x-rays.
MRI
MRI is useful in the assessment of soft tissue injuries including nerves, particularly intercarpal ligament injury or triangular fibrocartilage complex tears. It is also useful in the evaluation of occult fractures and avascular necrosis of carpal bones.
Treatment of Distal Radius Fracture
The treatment goal in fractures of the distal radius is a wrist that has pain-free motion and stability to permit vocational and avocational activities without the propensity for future degenerative changes.
Choice of Treatment – Nonoperative Vs Operative
The treatment of distal radius fracture has developed and changed drastically in the last two decades. However, the treatment still needs to be individualized and there does exist an area where the decision is dependent on surgeon assessment and patient’s demand than the guidelines.
The patient’s preinjury activity level is of utmost importance as the results are anchored to this. This is despite the age the patient belongs to. So the common notion that older people do not require anatomic reduction is vague. A 70 years old elderly person who participates in recreational sports like golf, hiking, and biking, etc. would require anatomic reduction whereas a patient who leads a sedentary life does not drive would be fine with a lesser reduction that allows return to full activities.
To bring objectiveness to the treatment, the following 3 parameters are of utmost importance. Following are the acceptable limits of these parameters in a demanding patient.
- Intra-articular Incongruity: Step-off should not be more than 1 mm. Some authors may accept up to 2 in certain cases
- Radial Length: Acceptable radial length is within 2 to 3 mm of the contralateral wrist. And not more than 5 mm in any case.
- Dorsal Tilt: The acceptable limit is up to the neutralization of the tilt but not more than 10 degrees in nongeriatric groups when compared to the opposite side. A value of more than 20 degrees indicates unstable injury.*
- Radial Inclination– Less than 5 degrees of loss is acceptable.
**It can be quite confusing to use the terms volar tilt and dorsal tilt. While the volar tilt indicates normal variation of radial articular slope as defined above, the dorsal tilt indicates dorsal angulation in case of fractures. The neutralization of the tilt would mean that there is a loss of the original volar tilt. A comparison to the opposite side makes things easier.
Nonoperative Treatment
The treatment with closed reduction and cast immobilization is indicated in stable distal radius fractures in which the treatment goals can be expected to be achieved and patients with low functional demands. The following fractures are suitable for nonoperative treatment.
- Extraarticular fractures
- Less than 5 mm radial shortening
- Less than 5mm dorsal angulation or <20 mm compared to the other side.
Nonoperative treatment consists of closed reduction and cast application.
Under suitable anesthesia, longitudinal traction is applied to the affected limb while the assistant provides countertraction. Direct pressure is applied to the displaced radial metaphyseal fragment for reduction. Whenever possible, reduction and cast application should be done under C-arm image intensifier control so that reduction can be confirmed. Otherwise, the reduction should be confirmed using plain X-rays after the maneuver.
The cast provides a dorsal buttress to prevent collapse. Excessive palmar flexion of the radius should be avoided to avoid the risk of acute carpal tunnel syndrome. If the ulnar styloid is intact, a short arm cast is enough in elderly people.
Postreduction x-rays are obtained at 7, 14, and 21 days. The postreduction x-rays must be compared with the initial postreduction x-rays to accurately determine displacement.
Operative Treatment
Following are the indications for surgical treatment of distal radius fracture.
- Comminuted displaced intra-articular fracture including articular margin fracture (dorsal or volar Barton fracture) and die-punch fractures
- Open fractures
- Associated carpal fractures
- Associated ulnar fracture
- Associated neurovascular injury or tendon injury
- Failed conservative treatment or displacement after closed treatment
- Bilateral fractures
- Impaired opposite limb
- Unstable fractures
- Concomitant ligamentous injury
- Greater initial displacement
- dorsal angulation > 5° (or > 20° of contralateral distal radius)
- displaced intra-articular fractures > 2mm
- radial shortening > 5mm
- Metaphyseal comminution
- Severe osteoporosis
When a patient with a distal radius fracture is a candidate for operative treatment, there are many surgical options to consider depending on injury and patient characteristics.
The optimal timing of the surgical intervention depends on the associated soft tissue factors and the type of surgical procedure
When a fracture is acute, the fracture should be reduced by closed reduction and the surgery should be carried out when the swelling is sufficiently reduced. In the case of minimal swelling, the surgery can be done immediately.
- External Fixation: Percutaneous pinning and plaster immobilization are unable to neutralize the axial forces. External fixation allows distraction across the radiocarpal joint and directly neutralizes axial load. External fixation alone may not be sufficiently rigid to prevent some degree of collapse and a loss of palmar tilt as good as an internal fixation. However, they provide good results with adjunctive fixation like supplemental bone grafts or K-wire fixation.
- Combined External Internal Fixation: This involves inserting pins into the distal metaphyseal fragment and attaching them directly to the external fixator resulting in improved mechanical stability and control over palmar tilt.
- Arthroscopically Assisted Reduction and External Fixation: Fractures that may benefit most from adjunctive arthroscopy are complex articular fractures without metaphyseal comminution and fractures with evidence of substantial interosseous ligament or triangular fibrocartilage injury but without a large ulnar styloid fragment. The procedure is usually performed between 3 and 5 days postinjury to allow healing of rents in the capsule to avoid extravasation of irrigation fluid.
- Open Reduction and Internal Fixation: Early range of motion of the joint, and avoidance of constrictive dressings or casts are major advantages of internal fixation but the technique is considered difficult and several soft tissue complications have been noted with the use of plate fixation. The plate can be either applied on a dorsal or palmar aspect of the radius. When applied on the dorsal aspect, the fixation provides a buttress against collapse and has the advantage of avoiding neurovascular injury [neurovascular bundle is on the palmar side]. However, extensor tendon ruptures due to prominent hardware and palmar displacement of the distal fragment have been noted. With palmar plating, the advantage of direct buttressing as in the dorsal side is lost but can be managed by the screw position in the distal fragment to buttresses collapse.
Complications
- Median nerve palsy: It is the most common complication with distal radius fracture and is seen more in high energy fractures. Avoiding excessive flexion and ulnar deviation can decrease the risk. It can be suspected by paraesthesia an weakness in thumb opposition. If required acute carpal tunnel depression may be done.
- Ulnar nerve neuropathy: It is less common than median nerve and the risk increases if there is a distal radio ulnar joint involvement
- Extensor pollicis longus rupture: It is thought to occurdue to tendon impingement, mechanical attrition or ischemia. Also associated with dorsal plate use.
- Flexor pollicis longus rupture: Seen with volar plating
- Degeenrative changes in radiocarpal joint: Associated with articular step off.
- malunion or Nonunion: Nonunion is rare in distal end radius fractures but malunion of varying degrees is seen. The treatment depends on the acceptance of the patient. An articular malunion needs to be addressed if the degenrative arthrosis is a risk.
- Compartment Syndrome: Needs to be recognized and addressed quickly
- Complex Regional Pain Syndrome: CRPS is a known complication of upper limb injuries and can be quite disabling. It needs multimodal approachfor its management.
Other Injuries of Distal Radius
Other injuries around the wrist injuries with a fracture of the distal radius are
- Radial styloid fractures
- Isolated volar lip fractures
- Isolated volar lip fractures
- Ulnar styloid fractures
Each of these injuries indicates a high-energy injury to the wrist and is discussed individually in different articles.
References
- Shehovych A, Salar O, Meyer C, Ford DJ. Adult distal radius fractures classification systems: essential clinical knowledge or abstract memory testing? Ann R Coll Surg Engl. 2016 Nov;98(8):525-531. [Link]
- Diaz-Garcia RJ, Oda T, Shauver MJ, Chung KC. A systematic review of outcomes and complications of treating unstable distal radius fractures in the elderly. J Hand Surg Am. 2011 May. 36 (5):824-35.e2. [Link]
- Ruch DS, Vallee J, Poehling GG, Smith BP, Kuzma GR. Arthroscopic reduction versus fluoroscopic reduction in the management of intra-articular distal radius fractures. Arthroscopy. 2004;20:225–30. [Link]
Some Images of Distal Radius Fracture








