Last Updated on October 31, 2020
Madelung deformity is an abnormality of the wrist caused by a growth disturbance volar-ulnar distal radial physis that causes
- Partial deficiency of growth of distal radial physis
- Excessive radial inclination and volar tilt
- Ulnar carpal impaction
The tilt in the distal radius is caused by inequality of growth. This leads to volar or palmar translation of the hand and wrist and causes a prominence of the distal ulna.
The deformity was first described by Otto W. Madelung whose name the condition bears.
The condition is known by many other names which are
- Carpus curvus Radius curvus
- Progressive subluxation of the wrist
- Manus valgus
- Manus furca
It is more common in the females and involvement is frequently bilateral.
Relevant Anatomy
Radius bone is a long bone that forms the radiocarpal joint with wrist bones.
[Read anatomy of distal radius]
Madelung deformity results in tilting of the radius and its relationship with the ulna.
An idea of normal articular surface and relationship can be evaluated if one knows the normal values.
Therefore the following measurements are important.
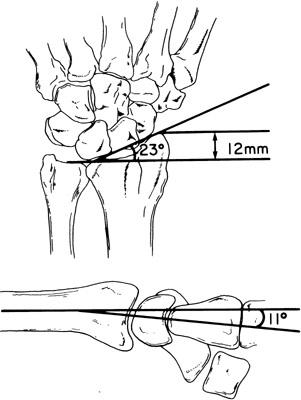
Radial inclination
This is the angle formed by a line from the distal radioulnar joint (DRUJ) to the radial styloid and a line perpendicular to the shaft of the radius through the lunate fossa; it is normally 21-23°
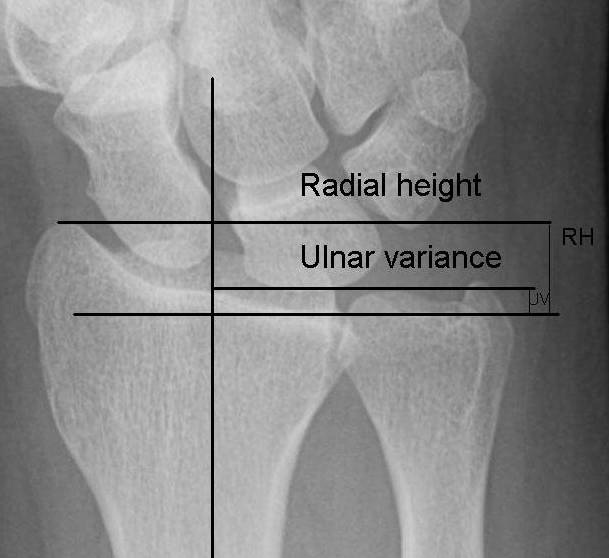
Radial length
This is the difference in longitudinal level between the lunate fossa and the radial styloid, which should be 12-15 mm
Volar tilt
This value is measured on a lateral view x-ray of the wrist. The angle formed between a line perpendicular to the radial shaft and a line through the dorsal and volar rims of the radial joint surface is called volar tilt. It is normally 10-15 degrees.
Ulnar variance
Ulnar variance refers to the difference between the levels of radial and ulnar articular surfaces. Normally, the articular surface lies slightly in distal position than the ulnar articular surface.
Pathophysiology of Madelung Deformity
The primary deformity is the bowing of the distal end of the radius, which is the most typical form curves in a volar direction while the ulna continues to grow in a straight line.
The distal ends of the radius and ulna are at different levels in the lateral plane. This is because the ulna has maintained its original normal position, while that of the radius has curved down to a volar side.
Growth disparity between ulna leads to the longer ulna and shorter radius resulting in negative ulnar variance. Normally, the distal articular surface of the radius is tilted 5 degrees toward its volar surface and 25 degrees toward the ulna, with its dorsal surface and radial margin convex and its volar surface and ulnar border concave.
Vickers ligament or radiolunate ligament is a fibrous band running from the distal radius to the lunate on the volar surface of the wrist may be accompanied by anomalous palmar radiotriquetral ligament. Some authors have suggested role of vicker ligament tethering in this deformity.
There are four types of Madelung deformity depending on the causation
- Post-traumatic
- Occurs following trauma
- Dysplastic
- Associated with bone dysplasias like
- Leri-Weill dyschondrosteosis [Most common association]
- Multiple hereditary osteochondromatosis
- Ollier disease
- Achondroplasia
- multiple epiphyseal dysplasias,
- Mucopolysaccharidoses
- Can be secondary to sickle-cell disease, infection, tumors, and rickets.
- Associated with bone dysplasias like
- Genetic
- 30% cases of Madelung deformity have autosomal dominant inheritance
- Turner syndrome has most common association
- SHOX gene is involved.
- Idiopathic
- No apparent cause or cause or association can be found.

There are two types of Madelung’s deformity.
- Typical, or regular
- Atypical, or reverse.
In the typical form, the distal articular surface of the radius may tilt toward its palmar surface as much as 80 degrees and ulnarward as much as 90 degrees.
In the normal wrist, the proximal row of the carpal bones is arranged in an arc, with its proximal surface forming a convex dome.
In Madelung deformity, this dome becomes peaked, its apex resting on the lunate bone. The radius and ulna are separated, with the peak of the carpal bones wedged into the interosseous space. The entire carpus is shifted toward the ulnar and volar side of the wrist.
A coalition of carpal bones may be present.

In reverse Madelung deformity is a rarer form.
In this, the distal end of the radius is tilted dorsally, reversing the plane of the distal end of the articular surface with a shift of the carpus toward the dorsal side. The distal end of the ulna then appears to be displaced volarly instead of dorsally.
Clinical Presentation
Most of the patients are symptomless before adolescence. Deformity of the wrist is the initial presenting complaint. It usually becomes obvious in late childhood or early adolescence, between the ages of 8 and 12 years.
There may be insidious onset wrist pain. Initially, it is minimal, disappearing on rest but may progress with deformity and ulnar resulted in ulnar impaction. With the progression of the deformity and impingement of the displaced carpus on the distal ulna, the pain increases. Pain is exacerbated by activity especially firm grip, pronation, and ulnar deviation of the wrist.
On examination, there would be ulnar causing a visible prominence on the dorsal and ulnar aspects of the wrist. The ulnar styloid end would be distal to the radial usually [negative ulnar variance].
The range of motion of the wrist is limited, especially in dorsal extension and ulnar deviation. Pronation and supination of the forearm are also limited.
As a rule, supination is definitely decreased, and pronation is impaired to a slight degree.
[In reverse Madelung’s deformity, palmar flexion of the wrist is decreased, while dorsiflexion is increased. The range of rotation of the forearm, especially pronation, is decreased.]
Median nerve irritation symptoms may be reported.
Imaging
X-rays
The deformity is characterized by
- Dorsal and radial bowing of the radius
- Undergrowth of the volar, ulnar corner of the radius
- Increased radial inclination
- Increased volar tilt
- Failure of ossification of the ulnar side of the distal radial epiphysis
- Carpal subluxation in a palmar and ulnar direction
- Lunate is gradually forced to the apex of the V-shaped radioulnarcarpal joint
- Dorsal subluxation of the distal radioulnar joint
- Wedging of the carpus between the radius and ulna
CT
CT scan provides better details of three-dimensional deformity though not necessary for routine treatment.
MRI
MRI can be done to assess Vicker ligament condition. to contemplate release of the same.
Treatment of Madelung Deformity
No treatment is required in asymptomatic cases though patient is kept under observation.
In cases of acute pain, activities are restricted especially which cause wrist impaction. Intermittent splinting may be done.
Surgery is indicated for the relief of pain and cosmetic improvement. The function is usually only minimally improved.
The decision of surgery is guided by
- Patients age and remaining growth potential
- Severity of deformity and symptoms
- Radiographic findings
Surgical procedures either correct the primary deformity of the radius or make a compensatory change in the ulna or both. The goal of ulnar procedures is to change the relationship of the relatively long ulna to the radius.
Different Surgical Procedures
Vickers physiolysis
When the deformity is noticed early and significant growth remains, changing the growth pattern of the distal radial physis to correct the deformity is possible.
The Vickers ligament originates on the radius in a fossa, is 5-7 mm thick and inserts into the anterior surface of the lunate and the anterior radioulnar ligament portion of the triangular fibrocartilage complex. This ligament could be a cause of pain in Madelung deformity.
Vickers ligament release is kind of physiolysis that may result in normal bony growth.
It is considered in patients with wrist pain or decreased range of motion efficacy and mild deformity in skeletally immature patients unknown.
The efficay is not established.
radial corrective osteomy +/- distal ulnar shortening osteotomy indications wrist pain or decreased range of motion cosmetic deformity functional limitations DRUJ arthroplasty indications highly controversial painful DRUJ instability and limited supination/pronation significant deformity may require staged procedures
Corrective Osteotomy of Radius
This is considered in the older child when remaining growth is insufficient. The osteotomy can correct the position of the distal radiocarpal joint surface and brings the radius and ulna into a more proper position. It could be closing or opening wedge osteotomy.
An ulna-shortening procedure can be performed along where required.
Ulnar Procedures
Because the radius is volar, the ulna appears to be subluxated dorsally and the incongruence at the distal radioulnar joint and impingement of the radius on the ulna in supination could lead to pain and stiffness.
Following ulnar procedures have been described to allow rotation. They can be done in combination to radial corrective osteotomy or done alone.
- Ulnar shortening
- Darrach Procedure
- Sauve-Kapandji procedure
- Fusion of distal radioulnar joint
Arthrodesis
This is considered in the skeletally mature patient who presents with pain and in whom physical examination demonstrates the limitation of motion and severe radiocarpal joint incongruity
Radiocarpal arthrodesis and distal ulna resection are indicated.
Complications
- Incomplete physiolysis
- Premature arrest of the growth
- Injury to radiocarpal or ulnocarpal joint
- Incomplete deformity correction
- Recurrent deformity
- Nonunion of the osteotomy site
Prognosis
Pain relief and correction of cosmetic deformity are the main goals of treatment and most of the patients attain both of them. The range of motion usually is only moderately improved at best.