Last Updated on November 22, 2023
The human shoulder is made up of three bones
- Clavicle or collarbone
- Scapula
- Humerus
Glenohumeral joint and acromioclavicular joints are the main joints of the shoulder region. The joints are stabilized by muscles, ligaments and tendons.
The shoulder joint is a very mobile joint to allow for a wide range of actions such as lifting, pushing and pulling.
Muscles of Shoulder
Muscles of the shoulder are responsible for movements of the shoulder region. They produce the characteristic shape of the shoulder.
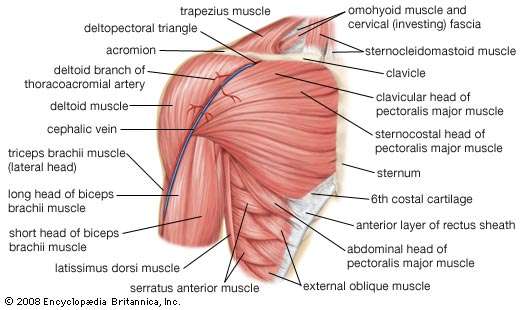
Image Credit: Britannica
Shoulder muscles are divided into two groups:
- Intrinsic
- Extrinsic
Intrinsic muscles originate from either scapula [mainly] or clavicle or both and attach to the humerus.
Extrinsic muscles of the shoulder originate from the torso and attach to either of the shoulder bones [clavicle, scapula or humerus].
The extrinsic muscles of the shoulder originate from the trunk and attach to the bones of the shoulder – the clavicle, scapula or humerus. They are located in the back and are also known as the superficial back muscles.
Pectoralis major and minor which are better known as pectoral muscles, also contribute and act on the shoulder.
Intrinsic Muscles of Shoulder
These are also called known as the scapulohumeral group of muscles. They originate from scapula or scapula and clavicle both or clavicle and insert on the humerus.
Following muscles are included in this group
- Deltoid
- Teres major
- Supraspinatus
- Infraspinatus
- Subscapularis
- Teres minor
The last four muscles, namely – supraspinatus, infraspinatus, subscapularis, and teres minor are commonly known as rotator cuff muscles.
The rotator cuff muscles are a group of four muscles that attach to the humeral head and. These muscles provide the glenohumeral joint significant stability.
In addition to their collective function, the rotator cuff muscles also have their own individual actions.
Deltoid
Deltoid muscle is the muscle that forms the bulk of the contour of the shoulder contour. It was previously called the deltoideus because it is in the shape of the Greek capital letter Delta.
It can be divided into an anterior, middle and posterior part.
Origin
Originate from the lateral third of the clavicle, the acromion and the spine of the scapula.
There are three discrete sets of muscle fibers,
- The anterior or clavicular fibers arise from the greater part of the anterior border and the upper surface of the lateral third of the clavicle. These are separated from the lateral part of the pectoralis major muscle by a small space that harbors the cephalic vein.
- Lateral fibers are also called acromial fibers. These arise from the superior surface of the acromion process of the scapula.
- Posterior or spinal fibers arise from the lower lip of the posterior border of the spine of the scapula.
Insertion
The fibers converge and insert on the deltoid tuberosity on the middle of the lateral aspect of the shaft of the humerus. Thus anterior fibers go obliquely backward, middle fibers come down almost vertically and the posterior fibers obliquely forward and laterally.
Though it is considered as a single insertion, it can be seen to have two or three discernible areas. The insertion has strong fascial connections anteriorly and posteriorly.
Blood supply
- Posterior circumflex humeral artery
- Deltoid branch of the thoracoacromial artery [a branch of the axillary artery.]
Nerve supply
The axillary nerve [C5 and C6], a branch of brachial plexus.
Function
- Anterior fibers – Flexion and medial rotation of the shoulder
- Posterior fibers – Extension and lateral rotation of the shoulder
- Middle fibers – Major abductor of the arm. The initial 15 degrees are conducted by supraspinatus, then these fibers take over.
It is important to understand the various interplays of different parts of deltoid and their interaction in movements with other movers of the shoulder.
Simultaneous contraction of all the fibers of deltoid muscle makes the deltoid muscle the prime abductor in frontal lane. The maximum effect is achieved in medial rotation of the arm.
By this, the deltoid stands out as antagonists to the pectoralis major and latissimus dorsi which act as adductor of arm.
Anterior fibers, however, assist the pectoralis major to flex the shoulder.
Acting along with the subscapularis, pectoralis and latissimus dorsi, the anterior fibers also act to internally rotate the arm.
The lateral fibers are abductors. These are also responsible for transverse or horizontal abduction.
The posterior fibers along with the latissimus dorsi to extend the shoulder.
The infraspinatus and teres minor along with the posterior deltoid as external rotators, and act as antagonists to internal rotators like the pectoralis and latissimus dorsi.
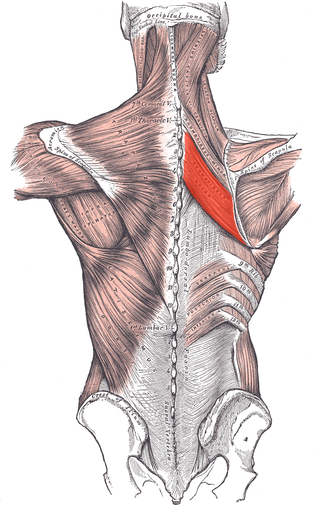
Teres Major
The teres major muscle is a thick flattish muscle. Teres means rounded in Latin.
Origin
The teres major muscle originates on the dorsal surface of the inferior angle and the lower part of the lateral border of the scapula.

Insertion
The fibers of teres major insert into the medial lip of the intertubercular sulcus of the humerus behind the insertion of the latissimus dorsi.
Nerve Supply
Lower subscapular nerve [C5-C8].
The thoracodorsal nerve provides the additional supply.
Function
The teres major is a medial rotator and adductor of the shoulder. It also helps the latissimus dorsi in drawing the previously raised arm downwards. It also assists in the extension of the arm and is a stabilizer of the humeral head in the glenoid cavity.
Supraspinatus
Supraspinatus is a muscle of the upper back that is one of the four rotator cuff muscles.
Origin
Supraspinatus originates from supraspinatus fossa on the posterior aspect of the scapula. It is separated from infraspinatus muscle origin [originates from infraspinatus fossa of scapula] by the spine of the scapula.
Insertion
It attached to the greater tubercle of the humerus.
Nerve supply
The suprascapular nerve (C5) a branch from the upper trunk of the brachial plexus. This nerve can be damaged along its course in fractures of the overlying clavicle, which can reduce the person’s ability to initiate the abduction.
Function
The supraspinatus muscle initiates the abduction of the arm and carries it from 0-15 degrees. After that deltoid takes over and becomes principal abductor and supraspinatus assists it till 90 degrees of the movement
Supraspinatus also pulls the head of the humerus medially towards the glenoid cavity.
It also prevents the head of the humerus to slip inferiorly.
Infraspinatus
Origin
Infraspinatus muscle originates from the infraspinous fossa of the scapula.
Insertion
It attaches to the greater tubercle of the humerus.
Nerve Supply
Suprascapular nerve.
Function
The infraspinatus is the main external rotator or lateral rotator of the arm.
When arms are fixed, it acts to adduct the inferior angle of the scapula.
The infraspinatus and teres minor, apart from being external rotators also extend the arm.
Subscapularis
Origin
Subscapularis originates from the medial two-thirds and from the lower two-thirds of the subscapular fossa of the scapula. [The subscapular fossa is a broad concavity on the costal surface of the scapula.]
The fossa in medial l two-thirds is marked by several oblique ridges. The ridges give rise to the tendinous part whereas and the surfaces between them give rise to the fleshy fibers.
An aponeurosis separates the muscle from the teres major and the long head of the triceps brachii.
Insertion
The fibers pass laterally to form a tendon that is inserted into the lesser tubercle of the humerus and the anterior part of the shoulder joint capsule.
Nerve Supply
Upper and lower subscapular nerves.
Function
The subscapularis is an internal or medial rotator of the arm. In a raised arm, it draws the humerus forward and downward.
Teres Minor
Origin
Teres minor originates from the posterior surface of the axillary border of the scapula in the upper two-thirds of its extent. It also originates from two aponeurotic laminae, which separates it from infraspinatus and teres major muscle.
Insertion
The fibers run obliquely upwards and laterally. The upper fibers insert into on the greater tubercle whereas lower just below that insertion by a distinct tendon.
Insertion
It attaches to the greater tubercle of the humerus.
Function
Teres minor is a lateral rotator of the arm. Along with infraspinatus, it also functions to hold the head of the humerus in the glenoid cavity of the scapula.
Teres minor is a weak adductor of the arm as well.
Nerve Supply
Axillary nerve.
Note on Rotator Cuff
Supraspinatus, infraspinatus, subscapularis and teres minor functions together to stabilize the head of the humerus by holding it in the glenoid cavity and preventing upward migration due to the pull of the deltoid muscle when the arm is elevated.
The four tendons of these muscles blend to form the rotator cuff tendon. Other structures like the articular capsule, the coracohumeral ligament, and the glenohumeral ligament complex also join before the insertion into tubercles of humerus.
Read more on Rotator cuff and rotator cuff injuries
Extrinsic Muscles of the shoulder
The muscles are organized into two layers – a superficial layer and a deep layer.
The superficial layer contains two muscles the trapezius and latissimus dorsi.
The deep layer contains three muscle levator scapulae and rhomboids major and rhomboids minor.
Trapezius

The trapezius is a large, flat and triangular muscle that extends longitudinally from the occipital bone to the lower thoracic vertebrae of the spine and laterally to the spine of the scapula. The muscles on each side form a trapezoid shape.
Trapezius is most superficial of all back muscles.
Origin
Trapezius takes origin from the posterior aspect of skull, nuchal ligament and spinous processes of C7-12 vertebrae
The details are as given below
Superior or upper fibers [Also called descending fibers]
- The spinous process of C7
- External occipital protuberance in the skull
- The medial third of the superior nuchal line of the occipital bone
- Nuchal ligament
Middle fibers, or transverse fibers
- The spinous process of C7, T1,2 and 3 vertebrae
Inferior or lower (or ascending) fibers
- Spinous processes of T4–T12
Insertion
- Superior fibers
- move downward and laterally to be inserted into the posterior border of the lateral third of the clavicle
- Middle fibers
- The medial margin of the acromion
- The superior lip of the posterior border of the spine of the scapula.
- Lower fibers
- Move upward and laterally to form an aponeurosis near scapula and inserts into a tubercle at the apex
Nerve supply
The accessory spinal nerve provides motor supply. It also receives proprioceptor fibers from C3 and C4 spinal nerves.
Function
Trapezius can cause movements of either scapula or spine when the other side is fixed.
The main function of the trapezius is to stabilize and move the scapula.
Upper fibers elevate, middle fibers retract and lower fibers depress the scapulae.
The trapezius is also a rotator of the scapula by action of upper and lower fibers to cause upward rotation bringing the acromion and inferior angles to move up. This is seen in the overhead movements of the arm.
[The levator scapulae and the rhomboids are rotators in opposite direction]
Trapezius fibers along with rhomboids act synergistically to cause scapular retraction/adduction.
When both scapulae are fixed, the trapezius muscles of both sides can act to extend the neck.
Latissimus Dorsi
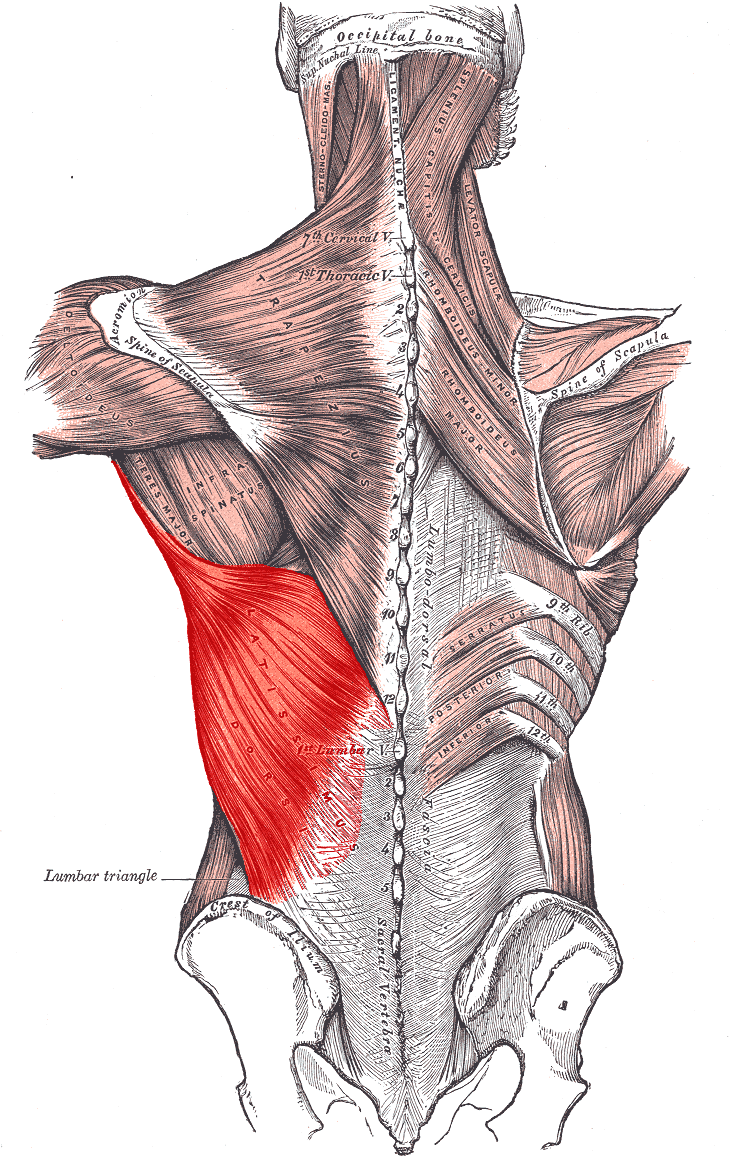
The latissimus dorsi which in Latin means the largest muscle is a large, flat muscle on the back that extends to the sides and behind the arm.
It is the largest muscle in the upper body.
Origin
Latissimus dorsi arises from
- Spinous processes of T7-T12
- Iliac crest
- Thoracolumbar fascia
- Inferior three ribs
Insertion
The fibers converge into a tendon that attaches to the intertubercular sulcus of the humerus.
Innervation
Thoracodorsal nerve [Long Scapular Nerve] [C6 and C7, C8].
Function
Latissimus dorsi extends, adducts and medially rotates the upper limb. It also assists in the extension and lateral flexion of the lumbar spine.
Levator Scapulae
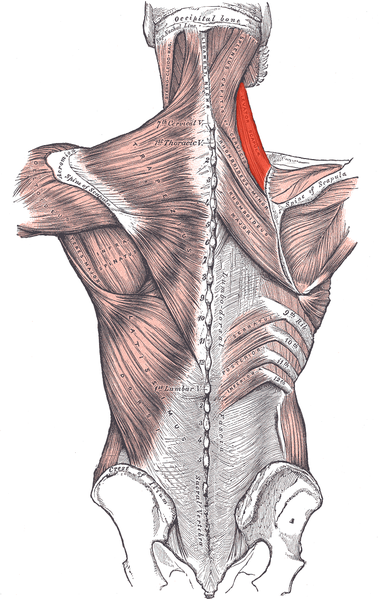
The levator scapulae is a small strap-like muscle which as the name suggests acts to elevate the scapula.
Origin
The levator scapulae originate from the posterior tubercle of the transverse process of the C1-C4 vertebrae.
Insertion
It inserts into the medial border of the scapula extending from superior angle to junction of the spine and medial border of the scapula.
Nerve Supply
The dorsal scapular nerve.
Function
Levator scapula elevates the scapula and rotates its inferior angle medially.
It also rotates the scapula down in conjunction with rhomboids and pectoralis minor.
When the shoulder is fixed, levator scapulae flex the cervical spine laterally. When both shoulders are fixed, levator scapulae acting together can flex-extend the cervical spine.
Rhomboids
There are two rhomboid muscles – major and minor. Both act together. The rhomboid minor is superior to the major.
Sometimes, both the muscles are fused together.

Rhomboid Major originates from the spinous processes of the T2-T5 vertebrae and is inserted on the medial border of the scapula, between the scapula spine and inferior angle.
Rhomboids minor originates from the spinous processes of C7-T1 vertebrae It inserts on the medial border of the scapula, at the level of the spine of the scapula.
Both the muscles are supplied by the dorsal scapular nerve.
Both act to retract and rotate the scapula.
These are also responsible for the downward rotation of the scapula with the levator scapulae, as well as the adduction of the scapula.
Clinical Significance
Rotator cuff tendonitis
Rotator cuff tendonitis refers to inflammation of the tendons of the rotator cuff muscles. This usually occurs secondary to repetitive use of the shoulder joint.
Accessory Nerve Paralysis
Iatrogenic cause [damage during the medical procedure like lymph node biopsy or surgery] is most common cause of injury to the accessory nerve.
The most common cause of accessory nerve damage is iatrogenic (i.e. due to a medical procedure). In particular, operations such as cervical lymph node biopsy or cannulation of the internal jugular vein can cause trauma to the nerve.
To test the accessory nerve, the trapezius function can be assessed.
Axillary Nerve Palsy
Axillary nerve can be injured in humeral fractures or injury due to injection injury. The deltoid muscle is wasted and the function of the abduction is affected
Injury
Muscle tears are less common and may affect deltoid and rarely teres major. Often the tendon injuries are more common and affect mainly the sportspersons.