Last Updated on October 28, 2023
Scapular winging or winged scapula refers to a dysfunction involving the stabilizing muscles of the scapula resulting in imbalance and abnormal motion of the scapula and causing protrusion or prominence of scapula bone.
Winging of the scapula is a rare but potentially debilitating condition that can affect the ability to lift, pull, and push heavy objects, as well as to perform daily activities of living.
It disrupts scapulohumeral rhythm and causes loss of power and limited flexion and abduction of the upper extremity.
It can also lead to cosmetic issues and though not often, it may result in pain.
Most of the cases of winged scapula involve the long thoracic nerve [supplies serratus anterior] and spinal accessory nerves [supplies trapezius] Rarely dorsal scapular nerve that innervates the rhomboid muscles may be involved.

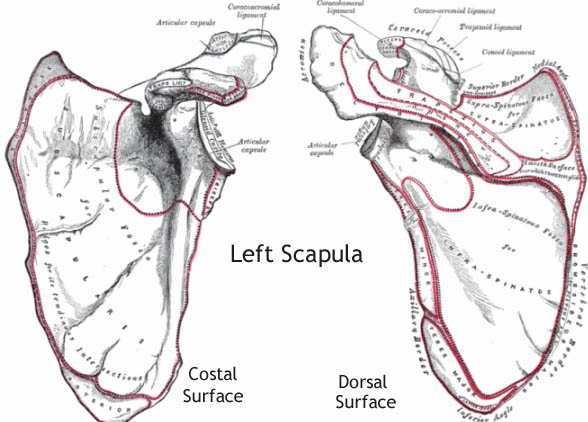
Relevant Anatomy
Scapulothoracic articulation is not a true joint but the bone is attached to thorax via ligaments at the acromioclavicular joint and stabilized by the muscles.
Serratus anterior and subscapularis muscles hold scapula closely to the thorax by creating a kind of suction while simultaneously allow the allows scapular movement against the posterior rib cage.
The motion of the scapula contributes to glenohumeral joint positioning and mechanics.
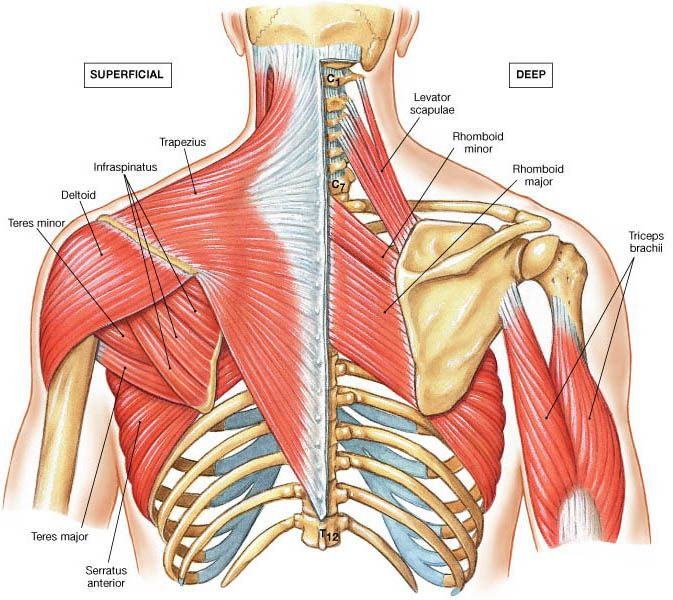
17 muscles attach to the scapula which functions to provide stability to the scapula, provide power to upper limb and synchronize glenohumeral motion by scapulohumeral rhythm.
- trapezius
- serratus anterior
- deltoid
- latisimus dorsi
- levator scapulae
- rhomboid major
- rhomboid minor
- omohyoid – inferior belly
- pectoralis minor
- teres major
- teres minor
- triceps brachii
- biceps brachii
- coracobrachialis
- infraspinatus
- subscapularis
- supraspinatus
The scapular muscles contribute to keeping the medial border of the scapula protracted against the posterior thoracic wall. The denervation or paralysis of any of these muscles results in the winging of the medial border of the scapula as it lifts off the thoracic wall.
In addition, the scapula may translate medially or laterally along the posterior thoracic wall due to unopposed muscle contraction of the other functioning scapular muscles, a distinction known as medial (serratus anterior paralysis) or lateral (trapezius or rhomboid paralysis) winging.
Most important muscles for the function of the scapula are given below.
Serratus Anterior
Serratus anterior originates from the first eight or nine ribs and inserts on the anteromedial border of the scapula. It has total 7-10 slips.
Its primary motion is scapular protraction (anterior and lateral movement). It is innervated by the long thoracic nerve which carries ventral rami of C5, C6, C7 from the brachial plexus.
It is supplied by long thoracic artery and branches of the thoracodorsal artery.
Functionally, it has three parts with different functions
- Upper part causes downward rotation (glenoid down) and stabilizes the superior scapula
- Middle part causes scapular protraction
- Lower part causes upward rotation and abduction
Trapezius
The trapezius is a large muscle that originates from the medial third superior nuchal line, external occipital protuberance, nuchal ligament and C7-T12 spinous processes and inserts on lateral third clavicle, acromion, and spine of the scapula.
Its primary motion is upward rotation and elevation of the scapula and is innervated by the spinal accessory nerve which is a cranial nerve [XI].
This muscle also has three parts with different functions
- Upper – Upward rotation and elevation
- Middle – Scapular retraction and adduction
- Lower – Downward rotation and depression
Rhomboids
Rhomboid major muscle originates from T2-T5 spinous processes and inserts onto the medial scapular border, just below the insertion of the rhomboid minor.
Rhomboid minor originates from C7 and T1 spinous processes and inserts onto the medial scapular border, near the base of the scapular spine
Both muscles function to cause scapular retraction and are innervated by the dorsal scapular nerve
Levator Scapulae
Levator scapulae muscle originates from C1-C4 transverse processes and inserts onto the medial border of scapula at the level of the scapular spine.
It elevates the scapula and also causes the downward rotation to tilt the glenoid cavity inferiorly.
It is supplied by C3-C4 cervical plexus with contributions from the dorsal scapular nerve.
Causes of Winging of Scapula
Winging may be caused by injury or dysfunction of the muscles themselves or the nerves that supply the muscles.
Loss of serratus anterior muscle function
- Occupational injuries causing serratus anterior paralysis
- Repetitive strain injury
- Seen in car mechanics, navy airmen, scaffolders, welders, carpenters, laborers, and a seamstress
- professional and amateur athletes
- Archery, ballet, baseball, basketball, bodybuilding/weightlifting, bowling, football, golf, gymnastics, hockey, soccer, tennis, and wrestling
- Nerve Lesions
- Traumatic injury
- Neuritis
- Compression
Loss of trapezius muscle function
- Radical neck surgery for tumors
- The spinal accessory nerve gets damaged
Weakness of all the scapula stabilizers
- Muscular dystrophies
- Facioscapulohumeral dystrophy most common
Brachial Plexus injury or disease
- Most of the nerves to the stabilizing muscles of the scapula arise from the Brachial Plexus. T
- Brachial plexus injuries
- Parsonage-Turner syndrome (Brachial Neuritis)
Loss of scapular suspensory mechanism [coracoclavicular ligaments]
- Dislocation of the acromioclavicular joint
- Fracture of the outer third of the clavicle
- Rupture of the coracoclavicular ligaments
- Scapulothoracic dissociation
These lead to an abnormal scapula rhythm and apparent scapula winging with overhead maneuvers. This is usually not painful and usually only affects overhead workers and athletes.
Secondary to instability
This is one of the commonest causes of scapula dysrhythmia (and winging). Recurrent dislocations of the shoulder lead to dysfunction of the muscles that move and support the shoulder complex and scapula.
An essential part of treating shoulder instability (recurrent dislocations) is treating the scapula dysrhythmia. This is done by an experienced physiotherapist in association with a shoulder surgeon.
Winging secondary to pain
This is another common cause of secondary winging and dysrhythmia of the scapula. Any painful condition of the shoulder will lead to abnormal movements of the entire shoulder complex. Reduced movement at the glenohumeral joint will lead to more compensatory movement at the scapula.
Types of scapular winging
Winging has been classified as medial or lateral depending on the direction of the superomedial corner of the scapula
Medial scapular winging
It is the more common type and is due to dysfunction of the serratus anterior. This muscle is supplied by the long thoracic nerve and affections of the nerve may also cause winging. It leads to the weak protraction of the scapula.
There occurs excessive medializing scapular retraction caused by rhomboids and elevation caused by trapezius leading to winging. It is more commonly seen in young athletes.
Medial scapular winging is caused by a deficit in serratus anterior function due to injury to the muscle itself or to the long thoracic nerve.
Common causes are
Mechanical
- Trauma to the serratus anterior causing avulsion
- Displaced fractures of the inferior pole of the scapula
Neural
Nerve traction injury is present in more than half of the cases.
The repetitive stretch injury is most common. It is characterized by a gradual onset of weakness and winging. The risk increases with activities involving head tilting during overhead arm activity, repetitive throwing, prolonged abduction. Commonly encountered in weightlifters, volleyball players.
Acute injury occurs in cases of high-energy trauma as in motorcycle accident. This leads to immediate scapular winging.
Compressive nerve injury could be acute or chronic.
An acute compressive injury is due to blunt trauma to the chest wall, head or neck. This might occur in contact sports or motor vehicle accidents. Falls may lead to this by causing sudden depression of the shoulder girdle.
Chronic nerve compression may be caused by compression at following sites
- Scalene muscles
- Subcoracoid
- Between coracoid and 1st or 2nd rib
- Often due to carrying heavy objects on the shoulder
- Inflamed bursae
- Subcoracoid
- Subscapular
- Supracoracoid)
- Anteroinferior scapular border
Direct injury to the nerve may occur in the following cases
- Iatrogenic
- Radical mastectomy/ axillary lymph node dissection
- Thoracic surgery
- Chest tube placement for pneumothorax
- Penetrating injury
- Brachial neuritis
- isolated unilateral palsy of the long thoracic nerve
Lateral scapular winging
This results mainly from the dysfunction of the trapezius. It is supplied by the spinal accessory nerve which is a cranial nerve. Loss of trapezius function caused weak superior and medializing force on the scapula and excessive lateralizing scapular protraction caused by serratus anterior, pectoralis major and minor occurs.
Deficit in trapezius function
It mainly occurs due to injury to the spinal accessory nerve. Its causes are
Iatrogenic [most common]
- Cervical lymph node biopsy
- Radical neck dissection
Traumatic
- Traction injury
- Sudden lateral flexion of the neck
- Motor vehicle or motorcycle accidents
- Blunt trauma – as in deep tissue massage
- Penetrating injury to the neck
Rhomboid palsy
These muscles are mainly affected by a dorsal scapular nerve palsy which can occur due to
- Nerve Entrapment
- Direct injury to the nerve
- C5 radiculopathy
Muscle injury during overhead athletics as in the motion of a pitcher or volleyball player can strain and injure the rhomboids.
Clinical Presentation of Scapular Winging
The presentation is similar both in medial and lateral scapular winging.
The patient presents with vague, nonspecific shoulder girdle pain and fatigue of muscles of the base of neck, scapula, and deltoid. Muscle spasms may be present.
There would be a weakness when lifting away from the body and overhead activity.
The patient may also complain of discomfort sitting against a chair.
Traction on brachial plexus may cause shoulder instability due to scapula failing to provide a stability.
Shoulder impingement may be seen in lateral scapular winging due to the inferior translation of the coracoacromial arch as scapula depresses secondary to loss of trapezius
On examination
The medial scapular winging
- The superomedial scapula elevates and protrudes posteriorly and medially. This protrusion is worsened by forward arm flexion.
- The abduction is often limited to 90° or less.
- There would be wasting of anterior scalene triangle due to atrophy of the sternocleidomastoid muscle. The weakness of forward arm flexion and abduction is seen
The lateral scapular winging
- the superomedial scapula drops downward and protrudes posterior and lateral.
- It is worsened by arm abduction and resisted external rotation
- The shoulder girdle appears depressed or drooping.
- There would be visible atrophy of the ipsilateral trapezius, weakness of forward arm flexion and abduction
Scapular stabilization manually improves manual stabilization of the scapula often improves pain in both types of scapular winging.
Diagnostic studies
Electromyography is the only study that can establish whether the cause is muscular or neural. It is also helpful in the nerve site involved.
Treatment of Scapular Winging
Medial Scapular Winging
Conservative treatment consists of
- Observation
- Physical therapy
- Activity modification
The observation is for a minimum of 6 months and ideally up to 2 years for the nerve to recover.
The patient should avoid painful or heavy lifting activities.
Physical therapy includes serratus anterior strengthening, stretching and bracing with a modified thoracolumbar brace can be considered.
Majority of patients will spontaneously resolve with full return of shoulder function and resolution of winging by 2 years
Operative Treatment
Early repair of serratus anterior avulsion
This is indicated in avulsion of the serratus anterior muscle.
Neurolysis of the long thoracic nerve
This is indicated when there is a failure to improve with conservative treatment taken at least 6 months and electromyography with signs of nerve compression.
The decompression is supraclavicular and is associated with better results than muscle transfers
Muscle transfer
This is considered when there is a failure to improve with conservative treatment, for 1-2 years and there is no nerve lesion.
Following transfers can be considered
- Split pectoralis major transfer [most effective]
- Pectoralis minor transfer
- Rhomboid transfer
Most important predictor of successful surgery is symptom relief and improved function with preoperative manual scapular stabilization.
Abduction weakness usually persists.
Muscle transfers may have complications like the failure of attachment at scapula, breast asymmetry in women and adhesive capsulitis
Nerve transfer
It is a microsurgery and indications are still developing.
The transfer could be of
- lateral branch of the thoracodorsal nerve to the long thoracic nerve
- medial pectoral nerve with sural nerve graft to the long thoracic nerve
The procedure has been shown to innervate the long thoracic nerve and provides the benefit of muscle preservation.
Scapulothoracic fusion
In this procedure fusion of the anterior scapula is done the posterior rib cage, with wire cables and/or plates and screws
It is often the last resort when treatments have failed. It is also considered in scapular winging from diffuse neuromuscular disorders.
The primary goal is pain relief though it also provides a limited increase in shoulder motion 20 degrees increase in abduction].
It is associated with complications like nonunion, adhesive capsulitis and symptomatic hardware.
Lateral Scapular Winging
The Conservative treatment approach is similar to the medial scapular winging and consists of observation, physical therapy, and activity modification.
However, the role of conservative treatment is controversial because most of the causes of lateral scapular winging are direct nerve injuries and warrant surgical intervention.
It can be considered in elderly and sedentary patients and those without an identifiable injury.
Inability to raise the arm above the shoulder at presentation and dominant extremity involvement is associated with poor outcome.
Surgical treatment consists of
- Exploration of the spinal accessory nerve, neurolysis, repair where nerve injury is identified. It should be preferably performed within 20 months of injury.
- Muscle transfer [ Eden-Lange transfer] is done when a nerve injury is diagnosed late (> 20 months after injury).
- The muscles transferred are the levator scapulae and rhomboid muscles.
- These are transferred from the medial border of the scapula to the lateral border for functional reconstruction of the trapezius muscle.
- Scapulothoracic fusion [see treatment of medial scapular winging for details] is considered as the last measure.
References
- Wiater JM, Flatow EL. Long thoracic nerve injury. Clin Orthop Relat Res. 1999;368:17–27.
- Foo CL, Swann M. Isolated paralysis of the serratus anterior: a report of 20 cases. J Bone Joint Surg. 1983;65:552–6.
- Fardin P, Negrin P, Dainese R. The isolate paralysis of the serratus anterior muscle: clinical and electromyographical follow-up of 10 cases. Electromyogr Clin Neurophysiol. 1978;18:379–86.
- Iceton J, Harris WR. Treatment of winged scapula by pectoralis major transfer. J Bone Joint Surg. 1987;69:108–10.
- Nakano KK. The entrapment neuropathies. Muscle Nerve. 1978;1:264–79. doi: 10.1002/mus.880010403.
- Friedenberg SM, Zimprich T, Harper CM. The natural history of the long thoracic and spinal accessory neuropathies. Muscle Nerve. 2002;25:535–9. doi: 10.1002/mus.10068.
- Disa JJ, Wang B, Dellon AL. Correction of scapular winging by supraclavicular neurolysis of the long thoracic nerve. J Reconstr Microsurg. 2001;17:79–84. doi: 10.1055/s-2001-12694.
- Okajima S, Tamai K, Fujiwara H, Kobashi H, Hirata M, Jubo T. Surgical treatment for spinal accessory nerve injury. Microsurgery. 2006;26:237–77. doi: 10.1002/micr.20239.