
Braces for scoliosis are recommended to prevent the scoliotic curve from getting worse. Many different types of braces are available now and can be used depending on the level, severity, and convenience of the person using them. Some braces for scoliosis are worn full time whereas others are night time only. Braces are used in scoliosis when the curve is not so mild that it could be managed … [Read More...] about Braces for Scoliosis- Types, Uses and Results
Main Content

Discogenic Back Pain Causes, Diagnosis and Treatment
Discogenic back pain is a common cause of axial low back pain [the pain is in the back as compared to radicular that that occurs in limbs as referred pain] without radicular symptoms. The condition is caused by damage to one or more discs. Relevant Anatomy The spine consists of stacked vertebrae that are connected by intervertebral discs anteriorly and facet joints posteriorly. The discs are … [Read More...] about Discogenic Back Pain Causes, Diagnosis and Treatment

Elbow Arthrodesis- Indications, Methods and Complications
Elbow arthrodesis refers to the surgical fusion of the elbow joint. It is not a commonly performed procedure in modern times. Historically, infection, mainly tuberculosis leading to a painful ankylosed elbow has been the main indication for performing elbow arthrodesis. But with modern chemotherapy, socioeconomic development has led to the reduction of tuberculosis drastically. Nowadays, … [Read More...] about Elbow Arthrodesis- Indications, Methods and Complications
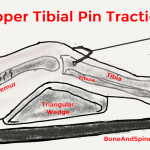
Skeletal Traction – Indication, Uses and Complications
Skeletal traction is a type of traction where the force is applied directly to the bone by inserting metal pins/screws in the bone. This is in contrast to the skin traction which applies the force on the limb through the skin surface. Traction is one of the oldest orthopedic treatment methods used for fracture, pain control, and deformity correction. With advances in surgical methods, the … [Read More...] about Skeletal Traction – Indication, Uses and Complications

Back Massage in Back Pain- Does It Help?
Have you ever considered a back massage for back pain? Do you wonder if it is really effective or would help you? Let us find out. Back pain and neck pain are often quite irritating and take time to go. Most of the back pains we have are due to postural abuse of the spine or degenerative changes in the spine. Modern medical treatment does not put much emphasis on massage therapy for back pain … [Read More...] about Back Massage in Back Pain- Does It Help?
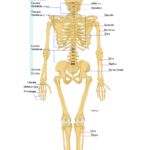
Classification of Bones and Its Significance
Classification of bones can be done in more than one way. It is important to understand the terms used so that confusion does not arise. Classification of Bones According to Shape Long bones Each long bone has an elongated shaft or diaphysis and two expanded ends (epiphyses) which are smooth and articular. The shaft typically has 3 surfaces separated by 3 borders, a central medullary … [Read More...] about Classification of Bones and Its Significance
Atypical Spinal Tuberculosis
Atypical spinal tuberculosis refers to the presentation of tuberculous disease of spine in a manner that is not usual presentation. The usual presentations of spinal tuberculosis have been discussed in great detail in the following article. Tuberculosis of Spine- Presentation, and Treatment Atypical spinal tuberculosis may involve other parts of the vertebra or it may affect the neural … [Read More...] about Atypical Spinal Tuberculosis
Improve Wellness to Prevent Orthopedic Ailments
We all strive to improve wellness and health but often keep postponing it. Today, we would look at the things we need to do to improve wellness and its impact on the reduction of orthopedic ailments. Orthopedics is a branch that deals in bones and joint disorders. This includes injuries, congenital malformation, wear and tear diseases like osteoarthritis, and other musculoskeletal … [Read More...] about Improve Wellness to Prevent Orthopedic Ailments

Scapulothoracic Bursitis Causes and Treament
Scapulothoracic bursitis is inflammation of the scapulothoracic bursae present between the scapula and rib cage. Symptomatic scapulothoracic bursitis is not very common. Another similar but different term used is scapulothoracic crepitus [snapping scapula] and it is important to highlight the difference. Scapulothoracic crepitus is referred to as thumping or popping sounds that occur with … [Read More...] about Scapulothoracic Bursitis Causes and Treament
Bursae Around Shoulder
There are 5-6 bursae around the shoulder. Bursae are the synovial fluid-filled sacs that are present between two surfaces that rub on motion. The purpose of the bursa is to reduce friction and protect the moving tissue. Often these are found at tendon-tendon and tendon-bone interfaces. There are five main bursae around shoulder. They include: Subacromial-subdeltoid bursa Subscapular … [Read More...] about Bursae Around Shoulder
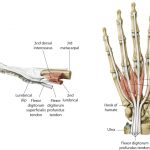
Dorsal Digital Expansion or Extensor Expansion
The term dorsal digital expansion refers to the small triangular aponeurosis covering the dorsum of the proximal phalanx with its base at the metacarpophalangeal joint. The main tendon of the extensor digitorum occupies the central part of the expansion and is separated from the metacarpophalangeal joint by a bursa. [Aponeurosis is a flat sheet or ribbon of tendon-like material that anchors a … [Read More...] about Dorsal Digital Expansion or Extensor Expansion
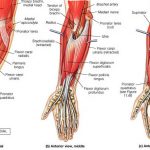
Forearm Muscles – Anatomy and Function
The forearm is the area of upper extremity between the elbow and wrist. The bony structure of the forearm is formed by two bones – radius and ulna. There are twenty forearm muscles which are arranged in two compartments – anterior and posterior. The anterior compartment contains flexor muscles and is also called the flexor compartment whereas the posterior compartment contains extensor muscles … [Read More...] about Forearm Muscles – Anatomy and Function

Head Halter Traction- Use and Complications
Head halter traction or cervical halter is a type of spinal traction used in cervical ailments and injuries. It is similar to skin traction used on the limbs and is based on the same principles. The head halter traction is provided by using head halter traction devices which produce an effect of stretching the neck vertebrae and muscles. Head halter traction is usually used for shorter … [Read More...] about Head Halter Traction- Use and Complications
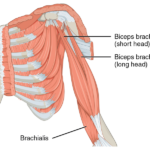
Muscles of Arm- Anatomy and Function
The region between the shoulder joint and the elbow joint is called the upper arm or arm. That between elbow and wrist is called forearm. Brachium and antebrachium are anatomical terms for arm and forearm respectively but are not used that commonly. Muscles of arm can be classified as that of a flexor compartment or anterior compartment [act to flex the elbow joint] and that of extensor or … [Read More...] about Muscles of Arm- Anatomy and Function

Muscles of Shoulder Region
The human shoulder is made up of three bones Clavicle or collarbone Scapula Humerus Glenohumeral joint and acromioclavicular joints are the main joints of the shoulder region. The joints are stabilized by muscles, ligaments and tendons. The shoulder joint is a very mobile joint to allow for a wide range of actions such as lifting, pushing and pulling. Muscles of Shoulder Muscles … [Read More...] about Muscles of Shoulder Region
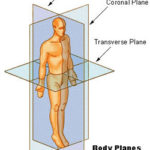
Anatomical Position, Planes and Locations
Anatomical Position of Human Body Anatomical position is the basic premise or central tenet, the very core on which all the details of anatomy are based. Thus, to understand the anatomy of the human body, the anatomical position has always to be remembered. The anatomical position of the human body is The person standing erect and face forward. Arms are straight along the sides of … [Read More...] about Anatomical Position, Planes and Locations
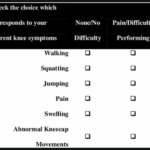
Anterior Knee Pain Scale- Use and Limitations
The anterior knee pain scale is a patient-reported assessment of symptoms and functional limitations in patellofemoral disorders. It was first published in 1993 by Kujala et al. The questions on the Kujala questionnaire add to total of100 points. Anterior knee pain results in significant symptoms and activity limitations. The anterior knee pain scale is a self-reporting tool. The other … [Read More...] about Anterior Knee Pain Scale- Use and Limitations
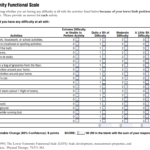
Lower Extremity Functional Scale – Method and Interpretation
Lower extremity functional scale is a test that consists of a questionnaire to evaluate the function of the lower limb in case of musculoskeletal condition or disorder. The test can be used to measure initial function, ongoing progress, and outcome. The lower extremity functional scale was developed in 1999 by Binkley et al. when they were evaluating a group of patients with musculoskeletal … [Read More...] about Lower Extremity Functional Scale – Method and Interpretation
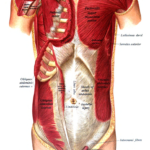
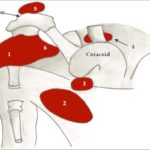
Muscles of Pectoral Region – Anatomy and Clinical Significance
Muscles of pectoral region or pectoral muscles are the muscles that connect the front of the chest to the bones of shoulder and arm. The pectoral region refers to the anterior chest wall. They are commonly called as pecs. These muscles also provide shape to the chest and pectoral exercises are quite famous among bodybuilders. The following four muscles constitute the muscles of pectoral … [Read More...] about Muscles of Pectoral Region – Anatomy and Clinical Significance

Rolando Fracture – Presentation and Treatment
Rolando fracture is a three-part intraarticular fracture-dislocation of the base of the thumb. This is an unstable injury that requires surgical reduction and fixation. It is named after Silvio Rolando, an Italian surgeon who described it first. Relevant Anatomy, Mechanism of Injury and Pathophysiology The carpometacarpal joint is between the base of thumb and trapezium bone. The … [Read More...] about Rolando Fracture – Presentation and Treatment