Last Updated on November 19, 2019
The hip joint is a ball-and-socket synovial joint which connects axial skeleton [pelvis] to lower limb [femur]. The ball of the joint is formed by femoral head, and the socket is formed by acetabulum. The acetabulum is formed by the merging of the ossification centers of ilium, ischium and pubis bones of pelvis.
The hip joint is designed to be a stable weight bearing joint. To achieve this, a large range of movement is sacrificed for stability. This is in contrast to shoulder joint where stability has been compromised for movement.
Bones of Hip Joint
Femur
The femur is the longest and heaviest bone in the human body. It consists of
- Proximal end,
- Shaft
- Distal end
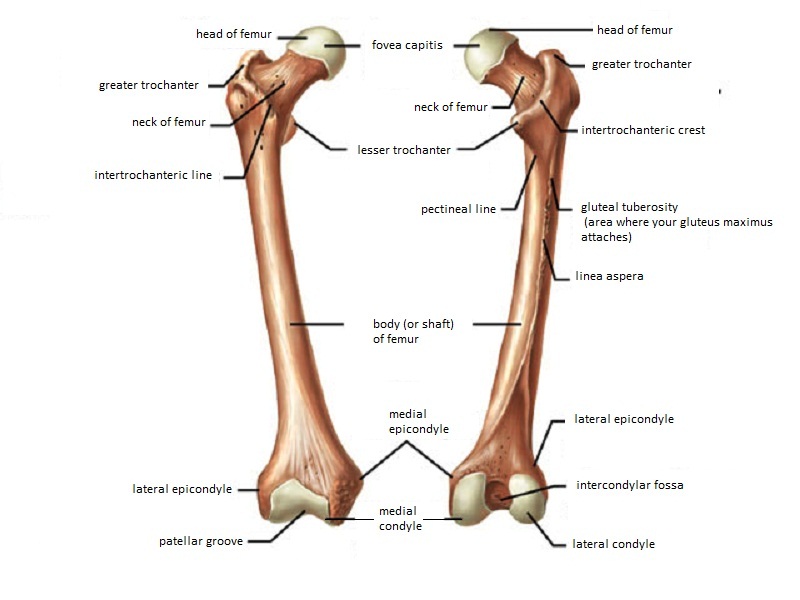
Its proximal end takes part in the formation of the hip joint. The proximal part consists of the head of femur, femoral neck, intertrochanteric region, and subtrochanteric region.
The femoral head is a dense mesh-work of trabecular bone and acts to facilitate the absorption and transmission of weight-bearing stress to the dense cortical bone of the femoral neck. The femoral head is almost spherical in shape and is surrounded by articular cartilage all around.
The femoral head size from roughly 40 to 60 mm in diameter and varies with body mass. Thickness of the articular cartilage is about 4 mm superiorly and tapers to 3 mm at the periphery.
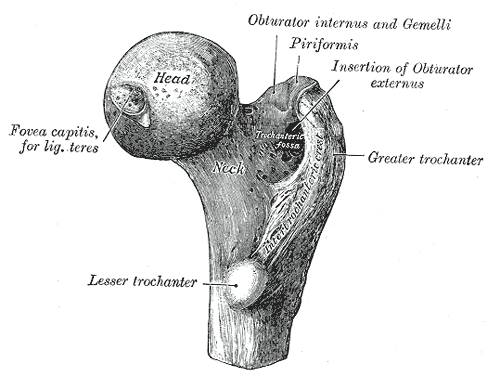
The femoral neck is the region between the base of the femoral head and the intertrochanteric line anteriorly and the intertrochanteric crest posteriorly.
The femoral neck forms an angle with the femoral shaft ranging from 125 to 140 [more at birth and decreases with age] in the anteroposterior plane and 10 to 15 degrees anteversion in the lateral plane.
Both superior and inferior borders of the neck of femur begin lateral to the femoral head, superior border ends distally at the greater trochanter and inferior border extends to the inferior trochanter. The superior border is shorter and thicker than the inferior border. The anterior surface of the neck is rough as compared to the head and the posterior surface has a concave appearance.
The cancellous bone of the femoral neck is organized into medial and lateral trabecular systems in response to the stresses on them. The medial trabecular system is in response to the joint reaction force on the femoral head whereas the lateral system resists the compressive force on the femoral head resulting from contraction of the abductor muscles.
The intertrochanteric region of the hip is a zone of transition from the femoral neck to the femoral shaft. This area is characterized primarily by dense trabecular bone that serves to transmit and distribute stress. This region contains the greater and lesser trochanters which are the sites of insertion of muscles.
The greater trochanter is a bony prominence on the anterolateral surface of the proximal part of the femur, distal to the femoral neck. The lesser trochanter is a bony prominence on the proximal medial aspect of the femoral shaft, just distal to the femoral neck. Iliopsoas inserts at lesser trochanter whereas greater trochanter serves as the insertion site for the gluteus medius and gluteus minimus. It serves as the iliopsoas insertion site.
The intertrochanteric line is a raised area that extends from the greater to the lesser trochanter anteriorly. This connection posteriorly is called the intertrochanteric crest, which contains the calcar femorale.
The calcar femorale is a vertical dense part of the proximal femur which extends from the posteromedial aspect of the femoral shaft to the posterior portion of the femoral neck. It is a kind of internal trabecular strut within the inferior portion of the femoral neck and intertrochanteric region for better stress transfer.
The subtrochanteric region extends from the lesser trochanter to an area 5 cm distal to it. It has dense cortical bone and is an area of high-stress concentration. It bears large compressive forces on medial aspect and tensile forces laterally.
Acetabulum
The socket of the hip joint is formed by a cup-shaped socket on the lateral aspect of the pelvis called acetabulum. The acetabulum is formed from parts of the ilium, ischium, and pubis.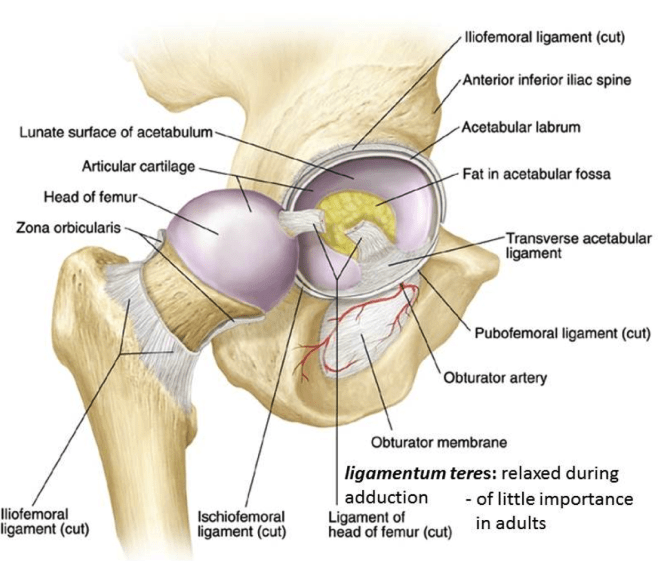
[For detailed anatomy of pelvic bones, read anatomy of hip bone]
The cavity of the acetabulum faces obliquely forward, outward, and downward. Acetabular labrum is a fibrocartilaginous rim like structure that functions to deepen the acetabulum to enable better holding of the femoral head. The margin of the acetabulum is deficient inferiorly. The acetabular labrum extends across this acetabular notch as the transverse acetabular ligament.
It prevents the femoral head from moving inferiorly by deepening the acetabulum inferiorly. It also converts acetabular notch into a foramen through which the nutrient vessels enter the joint.
Acetabular fossa is a rough depression in the floor of the acetabulum that is continuous with the acetabular notch. The lunate is the articular surface of the acetabulum to the femoral head.
At birth, each pelvic half consists of 3 separate primary bones: the ilium, the ischium, and the pubis joined by hyaline cartilage.
In infants and children, these large parts of the hip bones are incompletely ossified. At puberty, the 3 primary bones are still separated by a Y-shaped triradiate cartilage centered in the acetabulum. The primary bones begin to fuse at 15-17 years. Fusion is complete between 20-25 years of age.
These bones are discussed in greater detail in anatomy of pelvis.
Capsule and Ligaments of Hip Joint

The hip capsule is attached to the labrum and the transverse acetabular ligament, the medial side of the greater trochanter, the intertrochanteric line anteriorly, just superior and medial to the lesser trochanter, and the femoral neck posteriorly. Posteriorly, the fibrous capsule crosses to the neck 1-1.5 cm proximal to the intertrochanteric crest. The entire anterior aspect of the femoral neck and the proximal half of its posterior portion lie within the capsule of the hip joint. Fractures within this area are thus termed intracapsular fractures of the hip.
Some deeper fibers go around the neck, forming the orbicular zone, which holds the femoral neck in the acetabulum. The anterior capsule of the hip is the strongest and thickest part of the capsule.
There are two kinds of ligaments of hip joint – intracapsular and extracapsular. Ligament of the head of the femur is the only intracapsular ligament. Rest of the ligaments are extracapsular.
Ligament of head of femur is a small ligament that runs from the acetabular fossa to the fovea of the head of the femur. It also contains a branch of the obturator artery that forms a small portion of hip joint blood supply. It is also called ligamentum teres.
Extracapsular ligaments are three major ligaments (the iliofemoral, ischiofemoral, and pubofemoral) and one minor ligament (the zona orbicularis ) that conjoin with the hip joint capsule.
The iliofemoral ligament or Y ligament of Bigelow is the anterior ligament. It attaches to the anterior inferior iliac spine and the acetabular rim proximally. It courses in inferolateral direction and inserts on the intertrochanteric line distally. It is the strongest ligament. It prevents hyperextension of the hip joint during standing by holding the femoral head within the acetabulum.
The ischiofemoral ligament reinforces the hip joint capsule posteriorly. It originates on the ischial part of the acetabular rim and spirals superolaterally to the neck of the femur, medial to the greater trochanter. This ligament, like the iliofemoral, also prevents hyperextension and holds the femoral head within the acetabulum.
The pubofemoral ligament reinforces the capsule anteriorly and inferiorly. It begins from the obturator crest of the pubic bone and passes inferolaterally to join the fibrous capsule of the hip joint. This ligament prevents overabduction of the hip joint.
The zona orbicularis ligament consists of fibers that encircle the capsule at the femoral neck.
An iliopectineal bursa lies anteriorly over the gap in the ligaments, beneath the iliopsoas tendon.
Synovial membrane lines the capsule. It covers the neck of the femur between the attachment of the fibrous capsule and the edge of the articular cartilage of the head. It also covers the nonarticular area of the acetabulum, providing a covering for the ligament of the femoral head.
Retinacula are blood vessels containing deep longitudinal fibers of the capsule that goes superiorly from the femoral neck and blend with the periosteum. The bursa is considered the synovial extension beyond the free margin of the fibrous capsule onto the posterior aspect of the femoral neck.
A fat pad in the acetabular fossa is covered with a synovial membrane. It fills the acetabular area that is not filled by the femoral head.
The ligaments of the hip joint act to increase stability.
Blood Supply and Nerve Supply
Vascular supply to the hip joint is via the medial and lateral circumflex femoral arteries, and the artery to the head of femur.
The circumflex arteries are branches of the profunda femoris artery which is a branch of the femoral artery. They anastomose at the base of the femoral neck to form a ring, from which smaller arteries arise to the supply the joint itself.
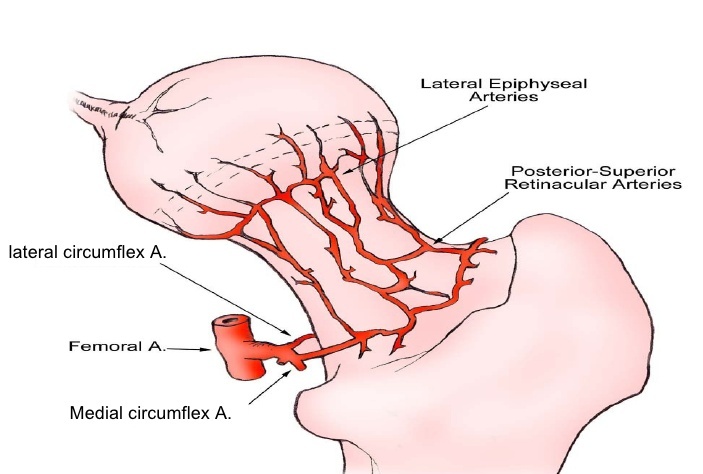
The medial circumflex femoral artery is responsible for the majority of the arterial supply (the lateral circumflex femoral artery has to penetrate through the thick iliofemoral ligament to reach the hip joint). Damage to the medial circumflex femoral artery can result in avascular necrosis of the femoral head.
The medial femoral circumflex artery, which originates from the medial or posteromedial side of the profunda femoris artery, runs posteriorly between the iliopsoas and pectineus and anastomose with descending branch of the inferior gluteal artery, the first perforating branch of the profunda femoris artery, and the medial and lateral circumflex arteries.
The hip joint is innervated by the femoral nerve, obturator nerve, superior gluteal nerve, and nerve to quadratus femoris.
- Genitofemoral nerve [L1-L2] supplies skin over the proximal anteromedial thigh.
- Obturator nerve [L2-L4] supplies the skin over upper inferomedial thigh.
- Lateral femoral cutaneous [L2-L3] suplies upper lateral thigh.
Muscles of the Hip Joint
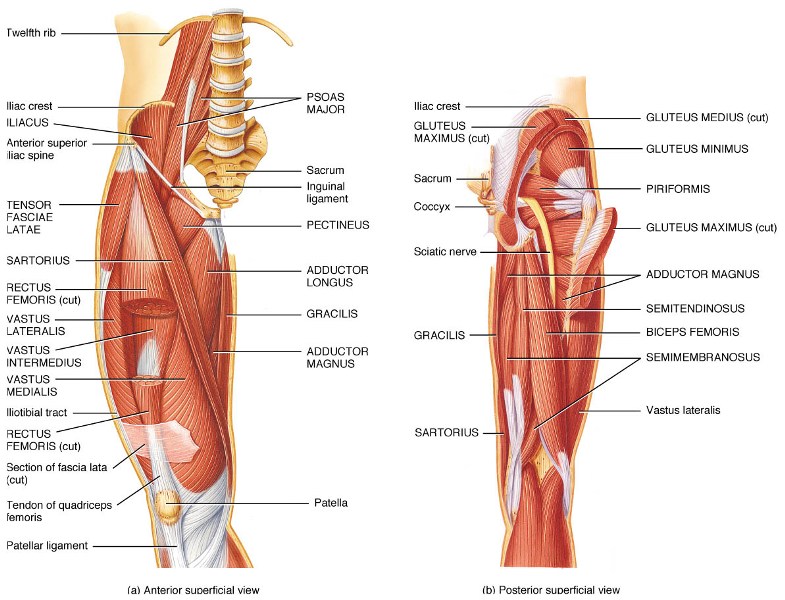
Sartorius
Sartorius, the longest muscle in the human body is a long, thin, band-like muscle that arises from the anterior superior iliac spine, descends obliquely across the hip joint and thigh and then runs medially and inferiorly to insert on the medial side of the tibia in the lower leg.
It functions as flexor, abductor and external rotator of the hip joint. At the knee joint the sartorius helps to flex the leg. Sitting cross-legged, making ankles rest on opposite knee are the movements where sartorius muscle is used.
Pectineus
It is a flat, quadrangular muscle that arises from the pectin pubis or the pectineal line and from the surface of the bone just in front of it. It inserts to pectineal line on femur and functions as an internal rotator.
Rectus Femoris
The rectus femoris constitutes quadriceps muscle along with vastus lateralis, vastus medialis, and vastus intermedius. It arises by two tendons: one, the anterior or straight, from the anterior inferior iliac spine; the other, the posterior or reflected, from a groove above the rim of the acetabulum.
The two unite and spread into an aponeurosis which is prolonged downward on the anterior surface of the muscle, and from this, the muscular fibers arise. The muscle gradually narrows into a flattened tendon and is inserted into the base of the patella.
Adductor Muscles
Adductor magnus , longus, brevis and minimus are adductor muscles of hip and originate as
- Adductor brevis arises from inferior pubic ramus
- Adductor longus Front side of the pubic bone under the pubic tubercle
- Adductor magnus Inferior pubic ramus and tuberosity of the ischium
- Adductor minimus Inferior pubic ramus
They all insert on medial ridge of linea aspera [A thickened ridge on posterior femur]
Tensor fascia Lata
The tensor fasciae latae is a tensor of the fascia lata, a fibrous sheath in the thigh. It arises from the anterior part of the outer lip of the iliac crest, anterior superior iliac spine, and part of the outer border of the notch below it and from the deep surface of the fascia lata.
It is inserted between the two layers of the iliotibial band of the fascia lata about the junction of the middle and upper thirds of the thigh.
The tensor fasciae latae tautens the iliotibial band and braces the knee, especially when the opposite foot is lifted.
Obturator Externus
The external obturator muscle is short external rotator muscle of hip joint. It is a flat, triangular muscle on the anterior wall of the pelvis.
It arises from two-thirds of the outer surface of the obturator membrane, the inferior pubic ramus, and the ramus of the ischium. The fibers converge and pass posterolateral and upward, to form a tendon that runs across the back of the neck of the and is inserted into the trochanteric fossa of the femur.
Obturator Internus
Obturator internus originates from the internal surface of the obturator membrane and posterior bony margins of the obturator foramen. It inserts on the medial surface of greater trochanter of the femur, in common with superior and inferior gemelli. It is a short external rotator of the hip joint.
Gemelli
The superior gemellus muscle arises from the ischial tuberosity and inserts on the greater trochanter. It is an external rotator of thigh.
The inferior gemellus muscle arises from the ischial tuberosity and inserts on the medial surface of the greater trochanter of the femur and rotates the thigh outward.
Piriformis
Piriformis is one of six short external rotators [others being superior gemellus, inferior gemellus, obturator internus, obturator externus, and quadratus femoris muscles – together known as depp gluteals] and participates on the abduction of hip also.
The piriformis muscle is found deep to the gluteus maximus and inferior to the gluteus minimus. It takes origin along the anterior region of the sacrum, extends laterally, passing through the greater sciatic foramen and crossing the hip joint to insert on the greater trochanter of the femur. Its name is because of its a pear-like shape.
Quadratus Femoris
The quadratus femoris is a flat, quadrilateral skeletal muscle located on the posterior side of the hip joint and is a strong external rotator and adductor of the thigh. It takes origin from ischial tuberosity and inserts into intertrochanteric crest.
Gluteus Medius and Minimus
The gluteus medius extends from the ilium to the femur and acts as abductor and medial rotator of the hip.
The gluteus minimus lies beneath the gluteus medius and is its companion in attachments and functions.
Both muscles lie beneath the superficial and largest of the posterior thigh muscles, the gluteus maximus.
Gluteus Maximus
Gluteus maximus is a large muscle of the hip that arises from the posterior gluteal line of the inner upper ilium, and the rough portion of bone including the crest, immediately above and behind it; from the posterior surface of the lower part of the sacrum and the side of the coccyx,lumbodorsal fascia, the sacrotuberous ligament, and the fascia covering the gluteus medius. The fibers are directed obliquely downward and lateralward.
The gluteus maximus has two insertions – iliotibial band of the fascia lata and gluteal tuberosity between the vastus lateralis and adductor magnus.
Hamstring Muscles
Semimembranosus, semitendinosus and biceps femoris are three hamstring muscles that originate above the hip joint and insert below the knee joint.
Semitendinosus and semimembranosus extend the hip when the trunk is fixed and flex the knee. They also medially rotate the lower leg when the knee is bent.
The long head of the biceps femoris extends the hip as when beginning to walk. Both short and long heads flex the knee and laterally (outwardly) rotates the lower leg when the knee is bent.
Gracilis
The gracilis muscle is a long, strap-like muscle that passes from the pubic bone to the tibia in the lower leg. It functions to adduct the thigh and to flex and rotate the leg medially at the knee.
Iliopsoas
The iliacus and psoas major muscles are closely related in structure and function and are often referred to as a single muscle, the iliopsoas. The iliacus arises from the ilium and the psoas major arises from the lumbar vertebrae. Both muscles merge to form a common insertion and inserts at the lesser trochanter of the femur.
Iliopsoas is the powerful flexors of the thigh at the hip joint.
Stabilizing Factors of Hip Joint
The primary function of the hip joint is to bear weight. The stability of the hip joint is offered by many factors.
The acetabulum is deep and encompasses nearly all of the head of the femur. The acetabular labrum increases the depth of acetabulum. The increase is depth provides a large articular surface, thus improving the stability of the joint.
The iliofemoral, pubofemoral and ischiofemoral are very strong ligaments and along with the thickened joint capsule, they stabilize the joint. These ligaments have a unique spiral orientation and this causes them to become tighter when the joint is extended adding stability to the joint.
Muscles and ligaments work in a reciprocal fashion at the hip joint. Posteriorly, where the ligaments are weak, the medial rotators are greater in number and stronger – they effectively pull the head of the femur into the acetabulum.
Movements of Hip Joint
The movements and their range at the hip joint are
- Flexion – 125°
- Extension – 10-15°
- Abduction – 45°
- Adduction – 30°
- Internal rotation – 40°
- External rotation – 45°
Flexion of the knee which relaxes the hamstrings, and increases the range of flexion to full.
Extension at the hip joint is limited by the joint capsule and the iliofemoral ligament. These structures become taut during extension to limit further movement.
Principle muscles responsible for those movements are
- Flexion: Iliosoas, rectus femoris, Sartorius
- Extension: Gluteus maximus, semimembranosus, semitendinosus and biceps femoris
- Abduction: Gluteus medius, gluteus minimus and the deep gluteals (piriformis, Gemelli etc)
- Adduction: Adductors longus, brevis and magnus, pectineus, gracillis
- Lateral rotation: Biceps femoris, gluteus maximus, and the deep gluteals (piriformis, gemelli etc)
- Medial rotation: Gluteus medius and minimus, semitendinosus and semimembranosus
Clinical Significance
Hip joint can be affected by many pathologies like osteoarthritis, rheumatoid arthritis. Trauma can result in fractures of the neck of femur, intertrochanteric fractures or subtrochanteric fractures of the hip. Hip joint can also get dislocated.
Hip joint replacement is a common surgery performed to replace the diseased or injured hip.